This case report presented the use of ISW (improved super-elastic Ti-Ni alloy wire, developed by Tokyo Medical and Dental University) in orthodontic treatment for an 34-year-old female patient who has skeletal Class I malocclusion combined with crowded upper anterior teeth, anterior crossbite, a missing maxillary maxillary canine and slight concave profile. In this case, mechanism including the use of reverse curve of ISW for dental crossbite correction, elastic chain for space closure, intermaxillary elastics for a better interdigitation, and substitution of maxillary first premolar for a missing canine were discussed. The total treatment time took 1 year and 7 months. Finally, after orthodontic treatment, an attractive profile was obtained and the patient was satisfied with the treatment outcome.
Dental crossbite involves localized tipping of a tooth or teeth and does not involve basal bone. A variety of factors have been reported to cause anterior dental crossbite, including lingual eruption path of the maxillary anterior incisors, crowding in the incisor region; and inadequate arch length. One of the most common etiologic factors for nonskeletal anterior crossbites is lack of space for the permanent incisors, therefore it is important to pay attention to the management of the total space analysis, not just to the crossbite during treatment planning[1-2].
Adult patients with anterior dental crossbite that compromise jaw movement may require orthodontic treatment. Various treatment methods such as removable acrylic appliances with finger springs and fixed orthodontic appliances have been proposed to correct anterior dental crossbite[3-6].
In this case, the use of ISW (improved super-elastic Ti-Ni alloy wire, developed by Tokyo Medical and Dental University) showed a simple and effective method for treating anterior dental crossbite.
A 34-year-old female patient came with a chief complaint of “unattractive smile due to the crowded dentition and anterior crossbite”. The extra-oral examination showed mild concave profile. The nasolzbizl angle was slightly obtuse (100°). The intraoral findings revealed upper anterior teeth crowding, dental crossbite and a maxillary canine missing.
The space analysis showed 8.0 mm of space deficiency in the upper dentition and 1.5 mm space deficiency in the lower dentition. Both upper and lower dental arches were symmetric ovoid shape (Figure 1). Panoramic findings showed #13 missing and #27 elongation (Figure 2). Cephalometric analysis indicated that this patient had a skeletal Class I pattern with an ANB angle of 3.4 ° with a mean mandibular angle. The upper incisor positions showed tendency of mild retroclination measured from U-1 to A-P plane of 5.3mm. The mandibular incisors were retroclined as compared to norms. (Figure 3, Table 1).


Figure 1: Before orthodontic treatment. Extra-oral photos and intra-oral photos.
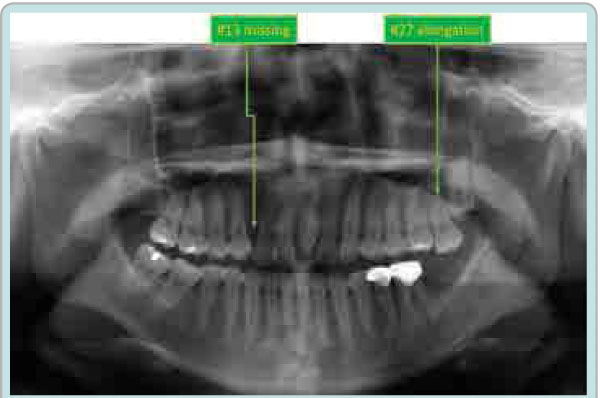
Figure 2: Initial Panoramic radiograph
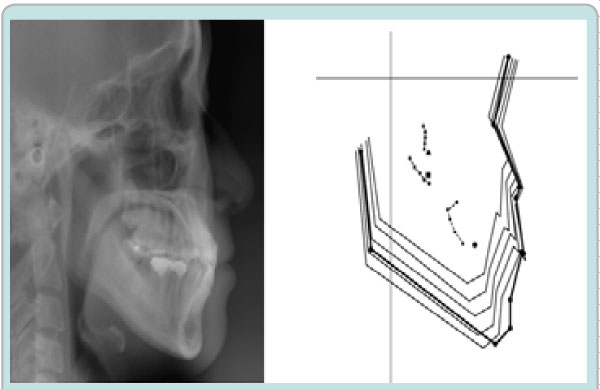
Figure 3: Initial Cephalometric radiograph
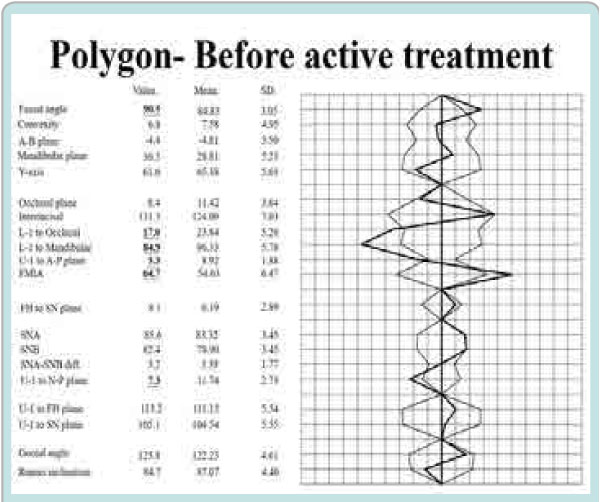
Table 1: Initial Cephalometric Analysis
Treatment objectives were addressed as:
According to this patient’s chief complaint, she wanted to have a beautiful and attractive smile as well as a stable occlusion after the treatment.
Therefore, the treatment plans were:
The initial leveling and alignment by 0.016x 0.022 ISW archwire were performed after full mouth direct bracket bonding (0.018inch pre-adjusted bracket). Then, correction of dental crossbite was done by using 0.016x 0.022 ISW archwire. Intermaxillary elastics were used for the establishment of intercuspal interdigitation. Finally, finishing and detailing were done with elastic chains. A stable occlusion and well aligned dentition were achieved.
The patient was satisfied with the treatment results after 1 year and 7 months of orthodontic treatment. (Figure 4, 5, 6 and Table 2)

Figure 4: After orthodontic treatment. Extra-oral photos and intra-oral photos.
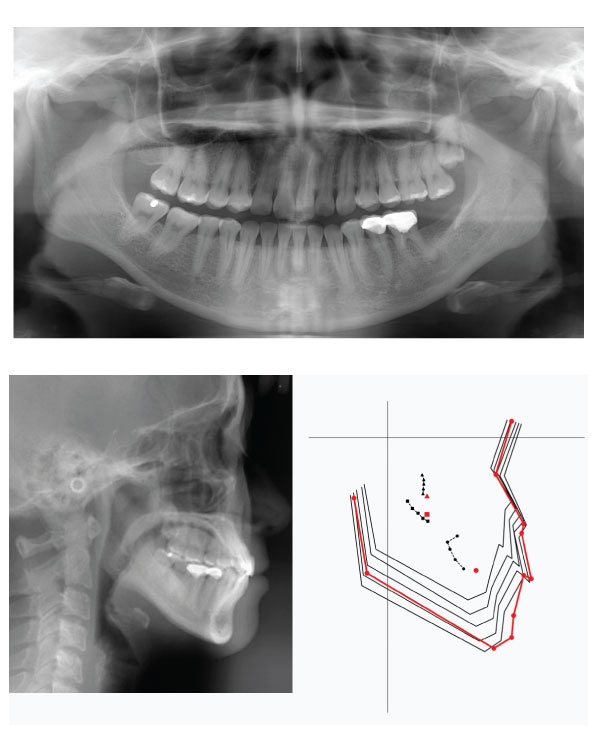
Figure 5: Post-treatment Panoramic and Cephalometric radiograph
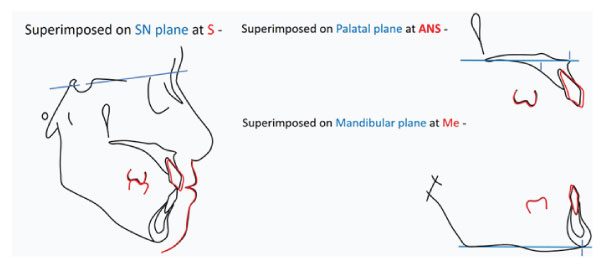
Figure 6: Cephalometric superimposition of initial (Black line) and post-treatment(Red line)
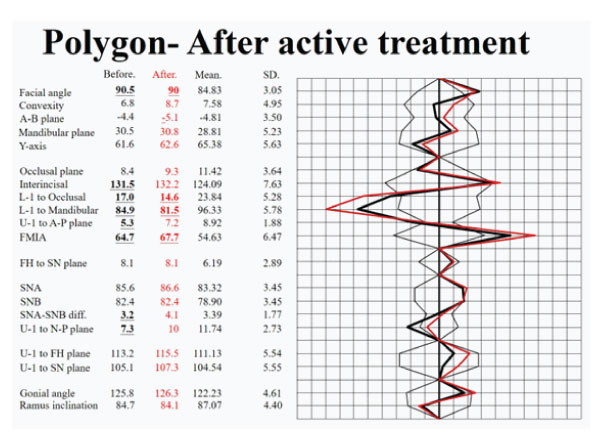
Table 2: Post-treatment Cephalometric Analysis
Dental crossbite correction
In this case, dental crossbite was corrected by ISW archwire leveling and expansion
within five months(Figure 8). When the ISW archwire was engaged into the bracket slots, the wire is not a straight line but a curvature, therefore the actual wire length(a+b) is longer than the straight line distance(c)[7-8] (Figure 9). This explains how arch expansion by leveling can be achieved. This is a simple and efficient approach for clinicians.
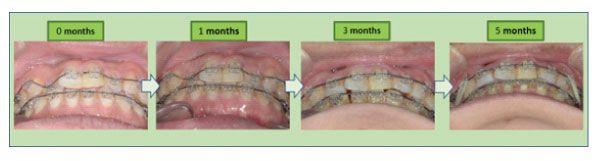
Figure 8:
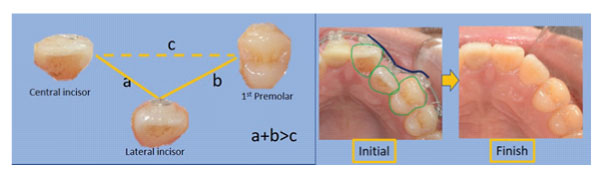
Figure 9:
In this case, the patient had a missing canine replaced with 1st premolar after the orthodontic treatment. There are some important factors that need to be taken into consideration during treatment planning, the details are as follows:
(1) Tooth morphology: When pre-adjusted appliances are used, it is advisable to use the corresponding bracket for each tooth to maintain the correct values of in and out and torque9. In this case, the canine bracket(0°) was bonded to #14 due to consideration of bracket integral torque(Figure 10).
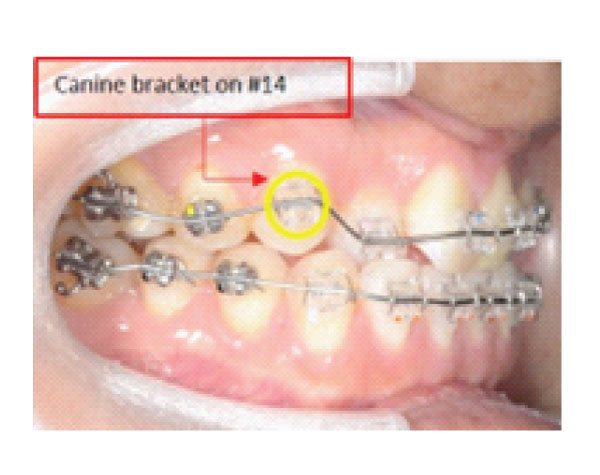
Figure 10:
(2) Tooth size discrepancy: The contra-lateral corresponding tooth size should be measured and taken as reference during anterior tooth alignment. Interproximal reduction may be necessary to eliminate size discrepancies. In this case, the first premolar width was reasonable, therefore no interproximal reduction was performed[10].
(3) Occlusal interferences: Root buccal torque was added for elimination of palatal cusp interference(Figure 11). There was no need for reduction of the maxillary premolar palatal cusps in this case, after cautious evaluation of the static and dynamic occlusion[11-12].(Figure 12)
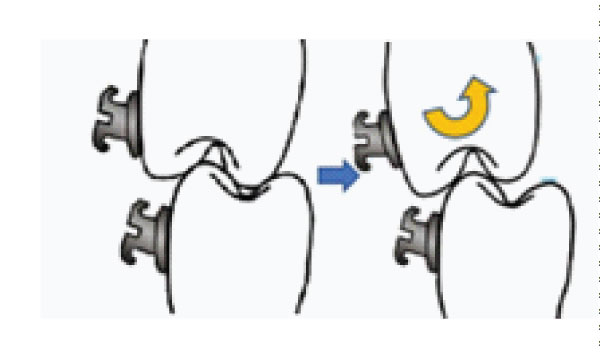
Figure 11:
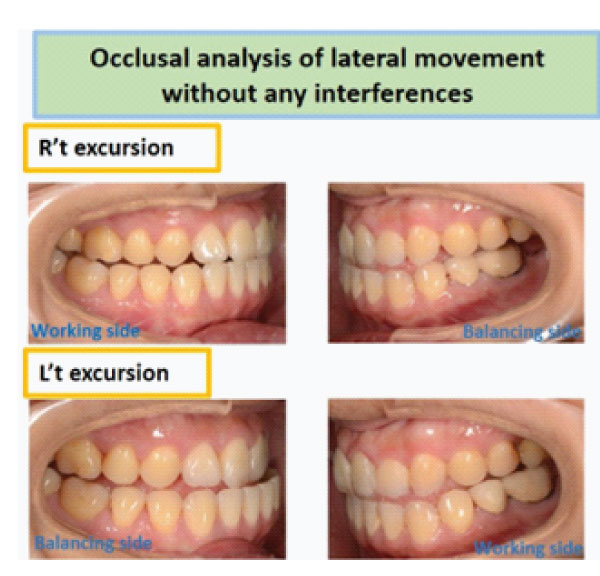
Figure 12:
In this case, canine relationship and good interdigitation were achieved within 6 months (Figure 13).
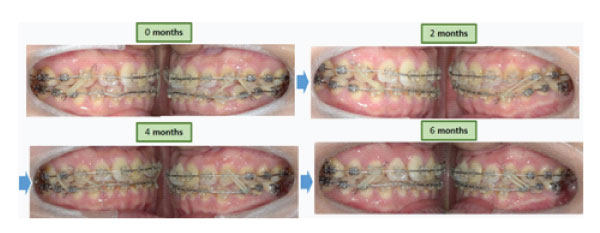
Figure 13:
When using intermaxillary elastics, there are some facts in the following that need to be kept in mind[13]:
(1) Amount of forces: The prescribed force is obtained when the elastic is stretched out 2.5~3 times its diameter. It is best to measure the elastic forces with a dynamometer to avoid excessive forces applied on the teeth.
(2) Force components: The direction of force causes favorable tooth movement or unfavorable side effects.
(3) Patient compliance: Patient education and motivation are important. “Elastics, they are working for you.”
This case report demonstrates the mechanism of dental crossbite correction and bite control by ISW with intermaxillary elastics, which led to a successful correction of the dental crossbite and achieved a pleasant profile after the treatment in a short period of time. The stability of the treatment was achievable even with the replacement of missing canine by first premolar and the treatment result showed stable, with no interference during the lateral movement of the mandible. In addition, canine substitution by 1st premolar can be an alternative treatment option for patients under such circumstances.