Data on risk assessment for ST elevation myocardial infarction (STEMI) in the immediate recovery period from COVID is lacking. Possible various pathogenic mechanisms of myocardial injury from COVID include hypoxia, inflammation in vasculature, cardiomyopathy, myocarditis, cytokine storm, demand ischemia (1, 2). Here we are presenting a case of STEMI in the immediate recovery period from COVID with no prior history of coronary artery disease and no prior significant risk factors for acute coronary syndrome (ACS).
Keywords: STEMI, COVID, Percutaneous Coronary Intervention, Acute Coronary Syndrome, Psychological Stress.
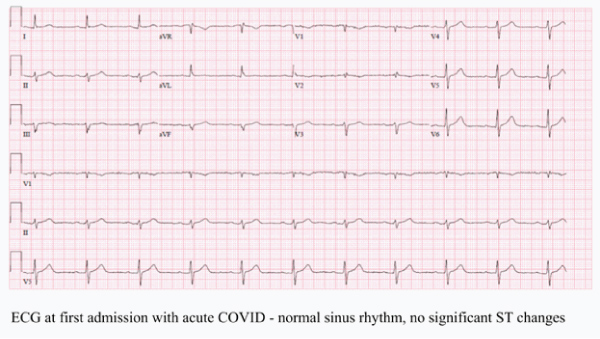
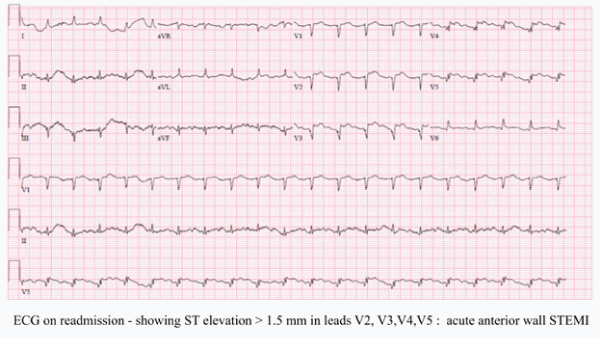
56 year old female with history of West Nile virus encephalitis with subarachnoid hemorrhage was initially admitted for COVID pneumonia with hypoxia requiring 2 L O2, has completed treatment with steroids, antibiotics and remdesivir for 5 days. She was weaned off oxygen and discharged home. Two days post discharge, she presented to the emergency room with dyspnea and chest pain. Chest pain is substernal without radiation ongoing for 2 hours prior to presentation without relieving factors. On exam hypotensive 90/50 mm hg, bilateral lung crackles present. Initial labs remarkable for troponin elevation at 4.3 ng/dl, ECG showed ST elevation greater than 1.5 mm in V2 , V3, V4, V5. Transthoracic echocardiogram showed EF 35 % with wall motion abnormality in anterior wall and no pulmonary embolism. She was diagnosed with acute anterior wall STEMI. She was given aspirin, clopidogrel and therapeutic anticoagulation with heparin infusion. She didn’t receive fibrinolytic therapy with a previous history of subarachnoid hemorrhage. Our center doesn’t have interventional cardiology and she was on waitlist for transfer for percutaneous coronary intervention (PCI). Unfortunately, she went into cardiogenic shock and subsequent cardiac arrest with unsuccessful cardiopulmonary resuscitation.
Cardiac complications in COVID include acute myocardial injury, heart failure, arrhythmias, spontaneous coronary artery dissection and sudden cardiac death. In our patient, she didn’t have any known risk factors for acute coronary syndrome prior to this COVID infection. In severe COVID with increased inflammatory response and cytokine storm increases the risk of plaque disruption causing ACS [1,2]. Patient family didn’t choose to do a post-mortem examination which could have been more informative in identifying and understanding COVID induced myocardial effects based on pathology findings in our patient. STEMI in COVID patients has high in hospital mortality compared to a STEMI patient who does not have COVID [3] due to various reasons including delay in providing appropriate care for revascularization with fear of contacting disease or spread of disease, multiorgan involvement in disease process, patient psychological stress, depression and availability of resources.
Identifying high risk populations for cardiac complications in COVID hospital admissions and close outpatient follow up after discharge and timely access to PCI if they have STEMI is key to prevent mortality. In our patient, although she didn’t have significant cardiac risk factors prior to COVID infection, immediate follow up post hospital discharge could have identified early presentation of acute coronary syndrome and might have improved her outcome if she was treated at PCI facility without delay. We have limited data on cardiac complications in the immediate recovery period from COVID, need more prospective studies and risk assessment tools to decrease morbidity and mortality.
None.
Author declare that there is no conflict of interest.