Eletrocardiographic signs of right ventricular sarcoidosis have been reported as precordial R‘ exceeding 1.65mm2, right precordial T-wave inversions and low voltage in limb leads. The question was how often right ventricular sarcoidosis can be suggested in a collective of definite, borderline or possible arrhythmogenic cardiomyopathy.
Methods: In a collective of 446 patients with arrhythmogenic cardiomyopathy (282 males, mean age 46.3 +/- 11.6 years) all cases with incomplete or complete right bundle branch block were analyzed with regard to precordial R` exceeding 1.65 mm2.
Results: In this special cohort right bundle branch block was found in 26 patients with prominent R waves in lead V1. In the 48 patients incomplete right bundle branch block with precordial R‘ wave in lead V1 in 3 patients. In all 4 patients precordial R‘ wave exceeds 1.65 mm2. T-wave inversions were found in lead V1 up to V3 in 4 patients with epsilon wave in lead V1 up to V3. 3 patients had low voltage in limb leads with atrioventricular conduction delay in two patient (PQ interval 220 and 240 ms, in the two other patients 190 ms).
Conclusion: Typical electrocardiographic criteria of right ventricular sarcoidosis was found in 4 patients (0.9%). Nearly all criteria were found: right precordial T-wave inversions, epsilon waves, atrioventricular block 1°, and low voltage in limb leads. In 3/4 patients arrhythmogenic cardiomyopathy could be excluded. PET CT is planned to confirm right ventricular sarcoidosis. With regard to standard ECG right ventricular sarcoidosis can be suggested with precordial R‘ abnormalities.
Keywords: Arrhythmogenic cardiomyopathy, right ventricular sarcoidosis, precordial R’ wave, right precordial T-wave inversions, low voltage in limb leads.
In some cardiac entities, the diagnosis can be made by simple standard ECG like long or short QT syndrome or brugada syndrome. In arrhythmogenic cardiomyopathy standard ECG is also a very important tool, but suspected diagnosis with multiple approaches are highly speculative. What is more important is the fact that imaging techniques such as echocardiography, right ventricular angiography or cardiac MRI as the best procedure are absolutely necessary for definite diagnosis. To distinguish right ventricular sarcoidosis new ECG criteria have been developed [1] with certain similarities to arrhythmogenic cardiomyopathy (right precordial T-wave inversions, low voltage in limb leads, and epsilon waves). In precordial ‘R’ wave, the area under the curve should be more than 1.65 qcm to diagnosis of cardiac sarcoidosis. The frequency of suggested ECG criteria in a collective of patients with definite, borderline and possible arrhythmogenic cardiomyopathy should be analyzed.
In a large collective of 440 patients (276 males, mean age 46.6 +/- 11.3 years) with definitive (n=375), borderline (n=58), and possible (n=7) arrhythmogenic cardiomyopathy 74 cases with complete and incomplete right bundle branch block were analyzed and in cases with precordial R‘ wave the area under the curve exceeding 1.65 qcm the diagnosis of right ventricular sarcoidosis was confirmed. The diagnosis of arrhythmogenic cardiomyopathy could be made by standard ECG, echocardiography, Holter monitoring, right ventricular angiography and later on cardiac MRI with gadolinium late enhancement, family history, and in a few cases genetic examination.
Four patients (0.9% of the whole collective) fulfilled the diagnostic criteria of cardiac sarcoidosis by standard ECG. Three cases were sampled from the possible form, one case from the definitive form of arrhythmogenic cardiomyopathy. In two cases arrhythmogenic cardiomyopathy could be excluded by cardiac MRI, in one case by direct view to the right ventricle in a surgical closure of atrial septal defect. The ECG‘s of the patients are presented (Figures 1, 2, 3, 4). Case no.1 was a 33-year old female patient who got surgical closure od atrial septal defect. Patient no.2 was a 54-year old female with syncope. Case no.3 is an 35year old male with non sustained ventricular arrhythmia. The last male patient, 20 years old, was missed for additional diagnostics. In this case, a definitive form of arrhythmogenic cardiomyopathy was obtained by epsilon waves in the ECG and right ventricular angiography. In Table 1 summarized ECG abnormalities in the four patients. Holter monitoring of all four patients revealed frequent ventricular extrasystole and non-sustained ventricular tachycardia.
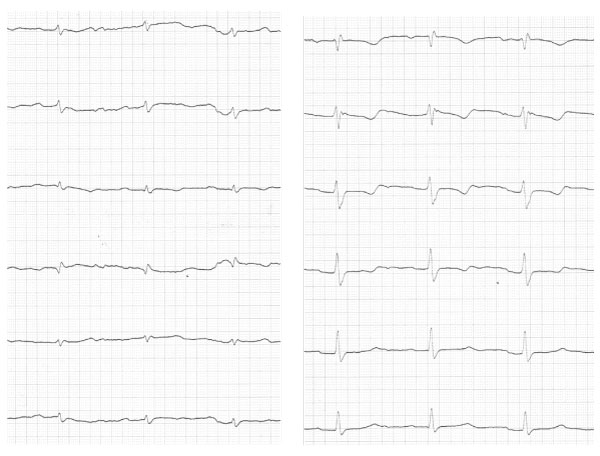
Figure 1: 33-year old female with atrial septal defect. In the ECG epsilon wave in lead V2, low voltage in limb leads, right precordial T-wave inversions, AV-block 1°, and QRS > 120msec.

Figure 2: 54-old year old female with non recurrent syncope. In the ECG PQ interval 190 msec, low voltage in limb leads, and right precordial T-wave inversions.
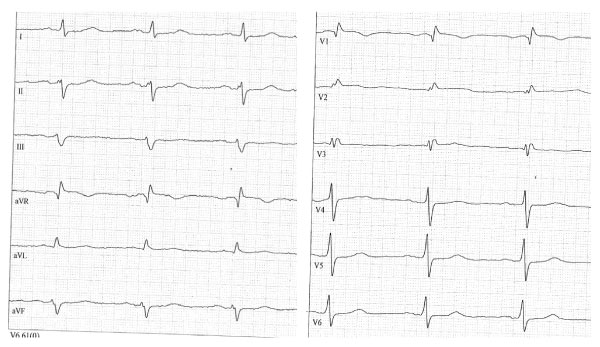
Figure 3: 35-year old male with non sustained ventricular arrhythmias. In the ECG right precordial T inversions, low voltage in limb leads, and slight ST elevation in lead V1.
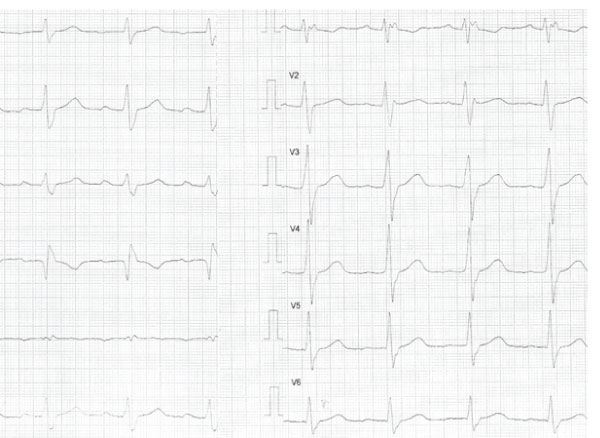
Figure 4: 20-year old male with non recurrent syncope. In the ECG right precordial T inversions, AV block 1°, and epsilon waves.
Table 1:
ECG abnormalities |
case no.1 |
case no.2 |
case no.3 |
case no.4 |
positive precordial R‘ |
+ |
+ |
+ |
+ |
ri.prec.T inversions |
+ |
+ |
+ |
+ |
low voltage limb leads |
+ |
+ |
+ |
+ |
PQ interval |
220 msec |
180 msec |
190 msec |
220 msec |
QRS interval |
120msec |
90msec |
80msec |
120msec |
In cases of right ventricular sarcoidosis myocardial biopsy or cardiac MRI obtains the diagnosis in only 25%. In cases of left ventricular involvement with reduced left ventricular function the diagnosis could be obtained by cardiac MRI and typical inferior late enhancement. For right ventricular involvement new ECG criteria were developed by 30 patients with right ventricular sarcoidosis and 30 patients with typical arrhythmogenic cardiomyopathy [1]. These criteria were used in a large collective of definitive, borderline, and possible forms of arrhythmogenic cardiomyopathy in order to get information of the frequency of right ventricular sarcoidosis that is 0.9% of the large collective. The rather low rate is obtained by largely sufficient discrimination of diagnostic criteria of arrhythmogenic cardiomyopathy. In general, cardiac sarcoidosis (left and right ventricular involvement) can be found at myocardial autopsy in about 10% [2]. In right ventricular biopsies or autopsies it is very difficult to find typical granulomas, exceeding to only 25% of cases.
In the four patients described, two had an exclusion of arrhythmogenic cardiomyopathy by cardiac MRI and one patient by direct view to the right ventricle during surgical closure of atrial septal defect. A PET-CT for confirmation of right ventricular sarcoidosis is planned for all of three patients. The fourth male patient with epsilon waves and angiographic right ventricular dilatation and local segmental aneurysms as major diagnostic criteria of arrhythmogenic cardiomyopathy was missed for additional diagnostic approaches in order to confirm the differential diagnosis of arrhythmogenic cardiomyopathy or right ventricular sarcoidosis. The patient has an event of non-recurrent syncope and in holter, monitoring a short episode of high-grade atrioventricular block appeared. This case is highly suspicious for right ventricular sarcoidosis, but could not be proven by cardiac MRI or PET-CT.
With the help of precordial R‘ abnormalities right ventricular sarcoidosis can be suggested in a low frequency in a collective of definite, borderline and possible arrhythmogenic cardiomyopathy.