Introduction: Variation in the assignment of diagnostic codes by physicians has multiple potential downstream results, including an effect on the use of these codes in the population of, and subsequent searches of patient databases for clinical research. As part of an institutional quality improvement project, we assessed variations in the use of the ICD-10 coding system between providers within a single academic pediatric orthopaedic group.
Methods: Coding data generated from October 2019 to January 2020 for outpatient clinical evaluations by three fellowship-trained pediatric orthopaedic surgeons were reviewed. ICD-10 codes were grouped by provider to determine total codes, most common codes, number of different codes per provider, numbers of injury and deformity codes, percentage of visits containing fracture codes, scoliosis codes, and percentage of visits containing pain codes. Two proportion Z-tests were utilized in order to compare injury and orthopaedic deformity percentages of total unique codes for each provider.
Results: During the study period, 1,091 clinic visits occurred, with utilization of 435 unique codes (1,444 total ICD-10 codes). 77% of visits contained only one code. The most common codes were T14.8XXA – non-specific fracture (185), M41.9 – scoliosis, unspecified scoliosis type, unspecified spinal region (42), and R52 – pain (40). There was a significant difference between providers regarding coding specificity, especially when generating codes for fractures (p=0.005) and scoliosis (p=0.005).
Conclusion: This study reveals statistically significant variability in ICD-10 coding within a single pediatric orthopaedic group in which all providers have similar practice profiles and areas of expertise. If generalized, this level of variation in coding may result in downstream effects on the reliability and utility of databases for large single or multicenter studies of pediatric orthopaedic patients or procedures.
The International Statistical Classification of Diseases and Related Health Problems (ICD) is an accepted standard for the identification and classification of medical diagnoses. The first edition of the ICD was adopted in 1983, and since then it has undergone numerous revisions, with each edition incorporating greater detail and specificity [1]. Use of the 10th edition (ICD-10) was made mandatory in the United States in 2015. In addition to the goal of providing accurate diagnoses for billing purposes, proper use of ICD coding has an important role in the generation of epidemiologic data and evidence-based medical decisionmaking.
Issues with the use of the ICD-10 coding system have been documented in the recent literature. Many of these reports have focused on the effect of the new system on large, multi-center registries that are sources of clinical information regarding total joint arthroplasty, and demonstrate that accurate and reliable use of the ICD-10 system can be challenging and complex. Multiple authors have demonstrated the potential implications in orthopaedic surgical research due to inaccurate use of the ICD 10 system within both hospital and administrative databases [2, 3].
There are few published reports of the effects of ICD-10 coding in Pediatric Orthopaedics. The goals of this study are to investigate the variability of diagnoses and conditions that are part of a fairly homogeneous academic pediatric orthopaedic practices, as well as to compare the ICD-10 coding practices of multiple providers with similar practice profiles within a single academic division. We hypothesize that there is significant variability in coding practices, as well as variance in the comprehensiveness of the coding between the providers.
This study underwent review as a potential institutional quality improvement project, and formal IRB review was deemed unnecessary. All outpatient clinic encounters performed by three pediatric orthopaedic surgeons at an academic medical center were reviewed from October 2019 to January 2020. All ICD10 codes for each encounter were queried from the electronic medical record. The data was sorted by ICD-10 codes, and provider, to determine the total number of codes, number of unique codes, most common codes, total codes per provider, number of different codes per provider, and percentage of codes with completion of all necessary elements. In addition, specific diagnostic codes for fractures, scoliosis, and pain were reviewed to assess the thoroughness of coding by the individual providers. Finally, the use of “unspecified” codes by each provider was documented. Two proportion Z-tests were utilized to compare injury and deformity percentages of total unique codes for each provider.
A total of 1,091 clinic visits occurred over the study period, and 1,444 total codes recorded. Records of most (77%) clinic visits contained only one ICD-10 code, 17% contained two codes, and 6% contained 3 or more codes. When comparing codes per provider, one provider accounted for a higher proportion of all reported codes (522 vs 460 vs 462), however the proportion of unique to total codes was not significantly different between providers.
The most common codes were T14.8XXA – fracture (185), M41.9 – scoliosis, unspecified scoliosis type, unspecified spinal region (42), R52 – pain (40), M41.125 – adolescent idiopathic scoliosis of thoracolumbar region (39), Q65.89 – developmental dysplasia of the hip (39), Z13.828 – scoliosis concern (35), Z98.890 – status post ORIF fracture (29), M54.5 – low back pain, unspecified back pain laterality, unspecified whether sciatica present (24), M79.672 – left foot pain (24), and M79.671 – right foot pain (21) (Table 1). The non-specific fracture code (T14.8XXA) was recorded in 16.84% of all encounters, and 81.52% of these fracture encounters had no other related ICD-10 codes to describe the fracture. Of all fractures coded, forearm fractures were the most common location of injury (33%, Figure 1). Significant discordance existed between providers regarding coding for fractures, as one provider used the non-specific code 54% of the time, which was significantly higher than the other two providers (38% and 41%, p=0.005 and p=0.042).
Scoliosis encounters accounted for 13.18% of all clinic visits. 22.92% of scoliosis encounters were coded as “scoliosis concern”. Lumbar scoliosis accounted for 2.08% of scoliosis encounters, 10.42% were “thoracic”, and 36.11% were “thoracolumbar”. 40.28% of scoliosis encounters were coded as “unspecified”. A similar coding discordance between providers existed for scoliosis: one provider used a non-specific code (M41.9) for 41% of scoliosis visits, which was significantly higher than the other two providers (16% and 19%, p=0.005 and p=0.036).
Table 1: Descriptions of the most common codes
Code |
Description |
Occurrences |
% of total codes |
T14.8XXA |
fracture |
185 |
12.2 |
M41.9 |
scoliosis, unspecified scoliosis type |
42 |
2.8 |
R52 |
pain |
40 |
2.6 |
M41.125 |
adolescent idiopathic scoliosis of thoracolumbar region |
39 |
2.6 |
Q65.89 |
developmental dysplasia of the hip |
39 |
2.6 |
Z13.828 |
scoliosis concern |
35 |
2.3 |
Z13.890 |
status post ORIF fracture |
29 |
1.9 |
M54.5 |
low back pain, unspecified back pain laterality, unspecified whether sciatica present |
24 |
1.6 |
M79.672 |
left foot pain |
24 |
1.6 |
M79.671 |
right foot pain |
21 |
1.4 |
Total |
478 |
31.5 |
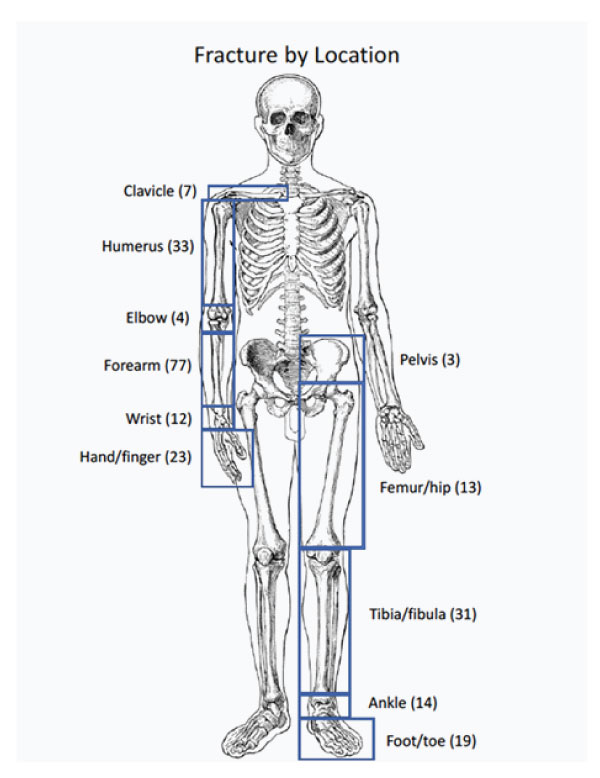
Figure 1: Fracture locations based on “S” group ICD-10 codes.
Pain-related encounters accounted for 3.6% of all clinic visits. Out of 40 encounters with the non-specific code for pain (R52), 18 of these encounters included no additional codes. One provider coded non-specifically for 63.6% of their pain encounters, which was grossly higher than the other two providers (33.3% and 41%) but not statistically significant (p=0.146 and 0.243). For pain encounters that included an additional code and thus were considered to be specific, the non-specific code for fracture (T14.8XXA) was the most common additional code (18.2% of specific pain encounters).
There were a total of 139 unique deformity codes and 296 injury codes between all providers. One provider included a significantly higher percentage of unique injury codes (60%) in the total number of codes when compared to the other two providers (39% and 45%, p=0.00001 and 0.0026). The other two providers did not differ significantly when compared to each other. When comparing percentages of unique deformity codes, there was a small, but significant, difference between two providers (26% vs 18% of total unique codes, p= 0.04). However, there was no significant difference between either of these providers and the third provider (23.6%).
There were also some codes that contained multiple descriptions. For example, 80% of the encounters that contained the code M92.8 were linked to “Sever’s Apophysitis” while 20% were linked to “Kohler’s Disease, Tarsal Navicular”. The code M92.51 was linked to “Osgood-Schlatter’s disease” 33.3% of the time and “Tibia Vara” for the other 66.6%.
The International Classification of Diseases and Health Related Conditions (ICD) system has been used as a source of diagnostic, and in some cases procedural, coding for over 100 years. The most recent update (ICD-10) was adopted internationally in 1994, but its implementation was not required in the United States until 2015. The most fundamental purpose of this system is to facilitate accurate tracking of diseases within patient populations, and it plays a significant role in the payment and financial infrastructure of healthcare systems worldwide. Most important to academic orthopaedic surgeons, ICD coding is used widely in searches of single and multi-site, as well as administrative and national, databases for the purpose of medical research.
The use of large institutional, national and international databases in orthopaedic surgery research has increased significantly over the last decade[4, 5]. The potential benefits of these databases are obvious, in that they allow access to data from large numbers of potentially diverse patients, and to assess the results of care and interventions over time. Use of databases as sources of studies for pediatric orthopaedics has become more common. Recent examples include review of statewide data for an epidemiological study of ACL injuries in skeletally immature patients [6, 7], the use of a multi-hospital database to assess the incidence of venous thromboembolism in pediatric patients after pelvic osteotomy [8] and multiple studies that query an international pediatric spine database to investigate natural history and interventions in patients with Early Onset Scoliosis [9, 10]. In each of these examples, ICD diagnostic and/or procedural codes were primary search criteria.
In the face of such widespread use, some authors have raised concerns regarding apparent issues and inaccuracies inherent in the use of such databases and have stressed the need for awareness of these shortcomings. Multiple studies have shown that dependence on coding data is a particular concern and potential source of error. Golinvaux, et al [5] demonstrated potential inaccuracies in the sensitivity of preoperative ICD-9 coding for anemia in adult spinal surgery patients at a large tertiary medical center. Recent studies reporting a decreased incidence of complications after total knee arthroplasty[11], as well one demonstrating concerns with changes in revision arthroplasty data [12], were felt to reflect the increased complexity and inaccurate usage of the newer ICD-10 system.
There is a dearth of literature regarding the use of ICD10 coding in pediatric orthopaedic surgery. Rabenhorst and Blasier [13] evaluated the adequacy of the new coding system to describe diagnoses found commonly in pediatric orthopaedic clinical practices. They found that while the ICD-10 provided more diagnostic options for pediatric orthopaedic conditions, there were instances of common conditions without a specific code in the new system, as well as dissimilar diagnoses that were defined by the same code. To date, no literature exists that specifically assesses the use of ICD-10 within in a pediatric orthopaedic practice by determining the level of variability in ICD-10 coding between providers in similar practice situations.
Results of this study reveal significant variability in the use of ICD-10 coding between 3 pediatric orthopaedic surgical providers within a single US academic institution. While the providers have similar practice profiles, there were significant differences in multiple areas of diagnostic coding. These differences included statistically significant differences between providers regarding unique injury and deformity codes. In addition, this assessment demonstrated significant differences, despite similar practice profiles, in the use of “non-specific” codes for both fracture patients and scoliosis patients. The variability in use of codes for a diagnosis of “pain” was also evident, but the differences between providers did not reach statistical significance during the sampling period.
These results raise important questions and concerns. First and foremost, they highlight the subjective nature of ICD coding. While changes to the system have been made with a goal of improving accuracy and specificity, this study shows that significant coding variability exists, even within a relatively small group of providers with similar practice profiles within a single academic department. The potential downstream results of this variability are numerous, both from academic as well as financial standpoints. These issues include concerns about the reliability of research dependent on patient information retrieved from databases utilizing coding queries, as well potential financial and/ or billing issues associated with the coding of both inpatient and outpatient clinical encounters.
Potential problems are foreseeable with the accuracy and reliability of clinical information due to wide variability of coding practices, which may occur even within a single pediatric orthopaedic practice. Significant differences, as shown in this relatively small study, may influence the reliability of patient information from local patient databases, as well as downstream issues if this patient data becomes part of multi-site national, international or administrative databases.