Field directed therapies (FDT) are used for the treatment of multiple actinic keratosis (AK), but recent publications suggest the possibility of induced tumours and cautious approach is needed.
In this study we assessed the behaviour of multiple AK on the scalp treated with cryotherapy and sun protection. Adults with more than five symmetrically distributed AK on the scalp were selected. The AK were counted, mapped, drawn, classified in grade I-II, photographed and Actinic Keratosis Area and Severity Index (AKASI) was calculated. At baseline the patients completed an auto-evaluation of sun protection use. They received grade II AK cryotherapy and were followed up for 6 months.
A total of 30 patients were included with a total of 557 AK and the overall response at 6 months was significant with 46% (155/557) of lesions cleared and AKASI decrease (p<0.05). The response per grade II AK treated with cryotherapy was 62%. All patients used hats outdoors. The use of sunscreen on the scalp did not add benefits.
Follow-up of patients with multiple AK on the scalp with sun protection and cryotherapy of grade II AK could be considered as a good option to manage, rotate and space treatments with FDT.
Key words :Actinic keratosis; Cryotherapy; Sun protection.
Studies of the treatment of multiple actinic keratosis (AK) with field directed treatment (FDT) without a control group have been published [1]. The exact behavior of the AK without FDT and the frequency of FDT application is not known1. Publications have suggested the possibility of induced tumors in the area treated with FDT and the mechanism action has not been established [2]. The evaluation of cautious approaches is needed.
On the other hand, cryotherapy is a safe, simple and costeffective treatment of AK present in all dermatological offices, and is the first choice of therapy for patients with a reduced number of AK [3].
To assess the behavior of multiple actinic keratosis on the scalp treated with sun protection and cryotherapy.
Patients
Adult patients with more than five symmetrically distributed grade I and/or II AK on the scalp were selected. Severe patients (AKASI > 8), patients with previous skin cancer or not always using a hat outdoors were excluded. Patients who had received FDT in the previous 24 months or on treatment with keratolytic creams on the scalp were not included. FDT comprised: Imiquimod (IMQ), 5-fluorouracil (5-FU), Diclofenac, Ingenol mebutate (IMB) and all variants of photodynamic therapy (PDT). The study was approved by the Ethics Committee of Ramon y Cajal hospital and conducted between May 2018 and June 2019. Diagnosis of AK was made by clinical assessment and dermoscopy. Demographic data of the patients such as sex, age and phototype were collected. The AK were counted, mapped, drawn and classified in grades I and II and photographed. The Actinic Kerastosis area and severity index (AKASI) was calculated. Also, at baseline the patient completed an auto-evaluation in a visual analogue score (VAS, 0-10) on sunscreen use.
Treatment protocol and response evaluation
Patients were evaluated at 3 and 6 months. Cryotherapy for grade II AK was applied in. two cycles of 10 seconds. At follow-ip the AK were counted, mapped and drawn again, and the AKASI was recalculated. The new AK, presented after the previous revision, were localized, counted and classified by grade.
The response to cryotherapy of grade II AK was assessed counting not only the total of AK but also per cryotherapy treated lesion.
Statistical analysis
Complete AK clearance was compared between groups using student t-test and 95% confidence interval (CI) assuming the independency between lesions. The total of AK (total and grades I or II) were divided into two groups depending on the use or nonuse of sunscreen. They were compared by using the two-tailed student t test with a significant value of p<0.05. The punctuation of 5 in the VAS was selected for dividing the patients according to the use of the sunscreen.
A total of 30 patients were included, all males, with a medium age of 77.23 (SD 4.99), a medium phototype of 2.13 (SD0.37) (Table 1) and with a medium AKASI of 4.37 (SD 1.59). A total of 557 AK were studied, 347 grade I and 210 grade II. The medium AK per subject was 18.57 (SD11.24), divided in 11.57 (SD 8.52) grade I and 6.70 (SD 4.88) grade II. Patients using sunscreen had a total of 317 AK with a medium AKASI of 4.17 (SD1.54), and a medium of 16.69 (SD 11.58) AK per subject. Patients not using sunscreen had had a total of 240 AK, with a medium AKASI of 4.73 (SD1.67) and a medium of 21.82 (SD10.33) AK per patient. Both groups were comparative at baseline (p>0.005).
Table 1: Patients demographic data and lesion characteristics at baseline
N=30 PATIENTS |
|
NO SUNSCREEN USE |
SUNSCREEN USE |
|
SEX |
|
|
|
|
Male |
30 (100%)) |
|
|
|
Female |
0 (0%) |
|
|
|
AGE (years) |
77.23±4.99 |
|
|
|
PHOTOTYPE |
2.13 (0.37) |
|
|
|
Total lesions per subject |
18.57 ±11.24 |
21.82 ±10.33 |
16.69±11.58 |
p=0.896 |
Grade I ± SD |
11.57±8.52 |
15.00 ± 7.01 |
9.58 ±8.80 |
p=0.525 |
Grade II ± SD |
6.701±4.88 |
5.82 ± 3.97 |
7.21 ±5.37 |
p=0.314 |
Total lesions (n) |
557 |
240 |
317 |
p=1.21 |
Grade I |
347 |
165 |
182 |
p=1.77 |
Grade II |
210 |
75 |
135 |
p=0.69 |
AKASI ± SD |
4.37±1.59 |
4.73 ±1.67 |
4.17± 1.54 |
p=0.896 |
VAS (0-10) use of sunscreen |
|
2.1 ± 2.0 |
8.84 ± 2.36 |
|
VAS (0-10) use of hat |
|
10 ± 0 |
10 ± 0 |
|
SD: standard deviation. |
||||
The overall response of the AK at three months was 34% (190/557) and was significative (p=0.00). The response of grade I was 38% (130/347, p=0.00) and grade II 29% (60/210, p =0.091) (Table 2). At three months, 68 new lesions appeared in the field (19%), 8% of which were grade I AK(18/217) and 33% were grade II AK(50/150). Among the 150 grade II AK at three months, 50 were new, and the response at three months per AK treated with cryotherapy was 48% (150-50/210, p=001). The medium AKASI at three months was 3.5 (SD 1.55, p=001), and decreased significantly from the basal AKASI (4.37, SD1.59).
Table 2: Overall, by grade and akasi response at 3 and 6 months, new lesions per revision by grade and response per lesion treated with cryotherapy.
|
RESPONSE |
P value* |
NEW LESIONS |
RESPONSE/LESION TREATED (P value) |
3 MONTHS |
||||
Overall |
190/557 (34%) |
p =0.000 |
68/367 (19%) |
|
Grade I |
130/ 347 (38%) |
p =0.000 |
18/217 (8%) |
|
Grade II |
60/210 (29%) |
p=0,023 |
50/ 150 (33%) |
150-50/ 210 (48%) (p=0.000) |
AKASI ± SD |
3.5 ± 1.55 |
P=0.001 |
|
|
6 MONTHS (with respect to basal) |
||||
Overall |
255/557 (46%) |
p= 0.001 |
127/302 (42%) |
|
Grade I |
193/347 (56%) |
p= 0.000 |
36/ 154 (23%) |
|
Grade II |
62/210 (30 %) |
p= 0.181 |
91/ 148 (62%) |
148-91/ 151 (38%) (p=0,001) |
AKASI ± SD |
3.39 ±1.37 |
P=0.002 |
|
|
The overall response of the AK at six months was significative (p=0,001) with respect to basal, with 46% (155/557) of lesions cleared, 56% response of the grade I AK (193/247, p=0.00) and 30% response of the grade II (62/210, p=0.18). At six months, a total of 127 AK appeared in the field (42%, 127/302), 36 were grade I AK(23%, 36/154) and 91 were grade II (62%, 91/148, p=0.000). Among the 148 grade II AK treated with cryotherapy, 91 (62%) were new, and the response per AK treated at the three months revision was 38% (148-91/151, p=0.000). The medium AKASI was 3.39 (SD 1.37) and decreased with respect to the basal AKASI (p =0.002).
No differences were found between patients using or not sunscreen but always wearing a hat are presented at baseline, at three and six months (Table 3, Supplementary material).
Table 3: Comparison in ak count and akasi with hat and hat plus sunscreen.
|
SUNSCREEN AND HAT |
HAT |
P value |
THREE MONTHS |
17. 28 (SD10.34) |
12.01 (SD 13.80) |
p=0.22 |
SIX MONTHS |
11.82 (SD9.65) |
11.55 (SD 10.60) |
p=0.95 |
The natural history of AK is regression and low risk of progression, and they are even a risk marker of no melanoma skin cancer (NMSC). There have been no publications reporting that AK treatment resulted in the reduction of NMSC [1].Thus, conservative treatments and follow-up is an option for the management of patients with multiple AK, especially in those with fewer than 10 AK, in which the risk of NMSC is low and the interval of FDT is not clear [1,3,4]. On the other hand, treatment with FDT requires the destruction of AK, and is sometimes painful, produces discomfort [2] and is expensive [5], even adjusted per AK treat [3,4]. Changing treatment is a real practiced approach strategy [1,3] and is cost-effective [5].
The aim of this study was to assess the behaviour of AK in the field without FDT. High risk patients were excluded, and patients selected were only followed for six months so as not to comprise other therapeutic options for them. Patients who always wear a hat covering the scalp were considered necessary to be included in the study to avoid sun exposure bias. The previous 24 months without FDT were considered sufficient to clear the interaction with the field. The AK were cautiously drawn and mapped to assess their exact location on the scalp and to notice if they were new or were previously presented at the revisions (Supplementary material, figure 1 and 2).
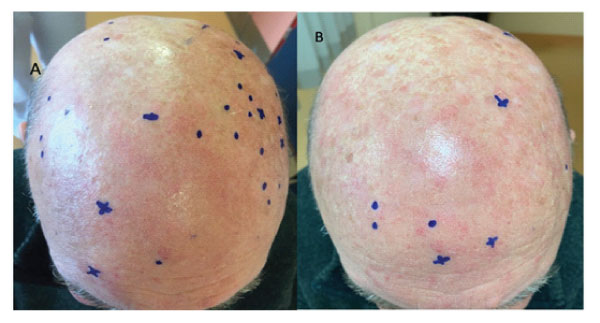
Figure 1:

Figure 2:
When AK in the scalp field were treated with sun protection and cryotherapy for six months, a total of 46% AK disappeared (p=0.001) with 38% complete response per AK treated with cryotherapy (p=0.001). But new AK appeared in the field with each revision, representing 42% of the total AK at six months, mostly by the growth of new grade II (62% of the total new AK). Curiously, at six months, grade I AK, treated only with sun protection in this study, decreased in number which was better than the grade II treated with cryotherapy (56% vs 30%). This is a small study, but these findings suggest that the role of sun protection could be important in these patients, particularly if they have multiple grade I AK, and the necessity of treating grade II AK. The evidence of the FDT in AK prevention is not high [1] and to our knowledge the studies published did not map the AK exactly, and further studies are necessary.
When corrected by lesion, the response of the AK to cryotherapy was significative with 38% of complete response (p=0.001), not as high as FDT, but randomized clinical trials comparing all treatments are lacking at this time [1,2,4].
AKASI decreased significantly and exhibited a good correlation with the total AK as only one area was evaluated [1].
The use of sunscreen did not add benefits in this group of patients probably because all of them always used a hat outside to protect the scalp from the sun (Table III, Supplementary material).
Many options are available for the treatment of AK and dermatologists should consider flexible regimens to avoid over treatment, but when multiple AK in the scalp are not treated they trend to gradually increase. Cryotherapy achieved 38% complete response per grade II AK treated at 6 months. Our data suggest that grade II AK need to be treated and grade I could improve with sun protection. Multiple AK in the scalp treated with sun protection and cryotherapy achieved significative response and could be include in rotational protocols to space FDT.
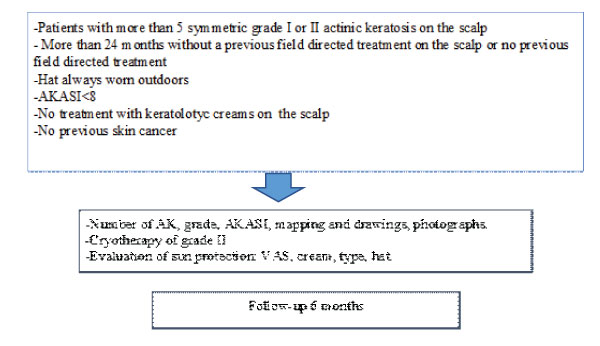
Figure S1: supplementary data
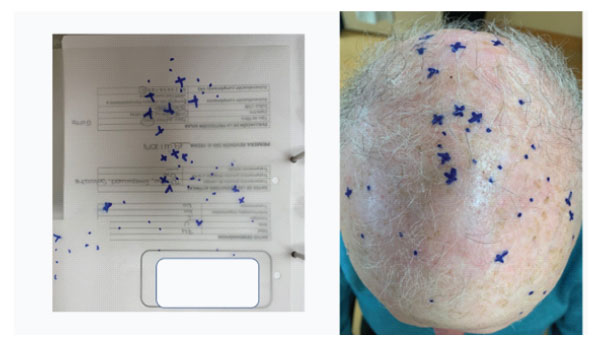
Figure S2: How the multiple actinic keratosis were follow-up.