Background: Retinopathy of Prematurity (ROP) is a condition confined to the premature retina. Hence, it is more commonly associated with extreme prematurity and low birth weight. Over the years, various risk factors have been explored to establish statistical correlation to help produce screening protocols to identify preterm infants most at risk of developing this condition.
Aim: The aim of our study was to evaluate risk factors, which may potentially lead to ROP.
Methods: The United Kingdom National neonatal computer system database (Badgernet) was searched for all babies born at Queen’s Hospital Burton using the eligibility criteria of gestational age of <32 weeks and/or birth weight <1501grams over a period of five years (Jan 2016 to Dec 2020). In addition, the local patient electronic health records were accessed to obtain further information about the course of illness.
Fishers exact test and logistic regression analysis was used to identify the link between the risk factors and the presence and severity of the disease. The P value of < 0.05 was taken as statistically significant.
Results: 207 fulfilled the inclusion criteria, 8 of them were later excluded due to death. Out of 199 babies studied, 17 developed ROP. The following risk factors displayed a statistically significant relationship with ROP positive patients: hypoxia, chronic lung disease, intra-ventricular haemorrhage, thrombocytopenia, anaemia, late onset sepsis, hypotension, patent ductus arteriosus, use of total parenteral nutrition, gestation less than 28 weeks and birthweight less than 1kg. Oxygen duration was significantly longer in ROP positive patients (p<0.0001). Similarly, both birthweight and gestational age were significantly lower in ROP positive patients (p<0.0001).
Conclusion: Our study confirms a strong correlation between ROP and prematurity/low birth weight. This study also adds useful information with statistically significant correlation with certain other important conditions/parameters that co-exist in these premature infants.
Keywords: Retinopathy of Prematurity, Preterm, Risk Factors, Gestational Age, Birth Weight
Retinopathy of prematurity (ROP) is a potentially blinding condition, confined to the immature retinal vascular system; it was first described in the 1942 as retrolental fibroplasia [1]. The likelihood of developing ROP is related to the stage of vascular development, which in turn relates to the maturity. Various risk factors for developing ROP including gestational age and birth weight, have been used to develop the clinical criteria for screening and treatment. Other risk factors had have been described in the literature and thought to have correlation with developing ROP and the severity of the disease.
Screening premature neonates for ROP was launched in the United Kingdom after the introduction of successful treatment. The Royal College of Paediatrics and Child Health (RCPCH), Royal college of Ophthalmologists (RCOphth), British Association of Perinatal Medicine (BAPM) and Bliss charity in conjunction with other stakeholders put together a national guideline for identifying which babies are at risk of ROP, describing a screening protocol and identifying criteria for treatment [2]. This guidance, which is under continuous update, is being used by 179 neonatal units in the United Kingdom, and annually reviewed within the National Neonatal Audit Programme (NNAP) [3]. World-wide, there are different screening programmes based on current identifiable risk factors. Most of these protocols are highly sensitive and, thereby result in screening of many infants who never develop clinically significant disease. In other words, significant over-screening is taking place, with all the burden of the cost it entails. Therefore, better understanding of risk factors will help to produce novel screening criteria to tackle this issue [4].
Recent advances in neonatal care have led to survival of more extreme premature infants with higher chance of developing ROP. Hence, regular regional and National review is critical in identifying new potential risk factors for these vulnerable infants. More recent studies have continued to show that the main correlation with ROP remains extreme prematurity, extremely low birth weight, intraventricular haemorrhage and pulmonary disease [5]. Some other studies have found that the risk factors linked to the development of ROP are different to the risk factors associated with disease progression [6]. In this study, we evaluated the local data over a 5-year period to study the correlation between various potential risk factors and the development of ROP.
The United Kingdom National neonatal computer system database (Badgernet) was searched to identify babies born at Queen’s Hospital Burton Upon Trent in Staffordshire. All babies born with gestational age of <32 weeks and/or birth weight <1501gram over a period of five years (Jan 2016 to Dec 2020) were retrospectively included in our study. In addition, the local patient electronic health records were accessed to gather further information about their course of illness. ROP screening dates, outcomes and subsequent treatment provided for each baby was also recorded.
Fishers exact test and logistic regression analysis was used to identify the link between potential risk factors and the presence and severity of the disease. P value of < 0.05 was taken as statistically significant.
207 eligible babies were originally recruited in the study. 8/207 (3.9%) babies died during their stay on the neonatal unit and were later excluded from further analysis. 199 remaining babies were further studied in detail. 17/199 (8.5%) babies developed ROP (10 males and 7 females) while 182/199 (91.5%) were ROP negative (Figure 1) with 108 males and 74 females. 5/17 (29%) ROP +ve babies required laser therapy.
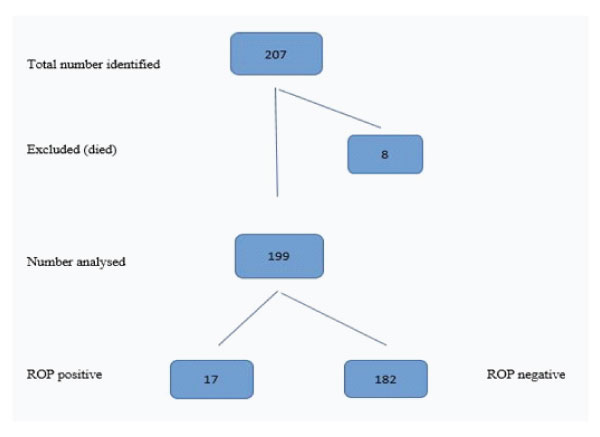
Figure 1: Number of cases analysed during the study.
Birthweight as well as gestation were statistically significantly lower in ROP positive patients. Mean birth weight in ROP +ve babies was 833 g (CI = 710-958 g) while it was 1342 g (CI = 13001385 g) in ROP -ve babies ( P = < 0.0001). Mean gestation in ROP +ve babies was 26 weeks (CI = 24.7-26.3 weeks) while it was 30 weeks (CI = 29.7-30.1 weeks) in ROP -ve babies ( P = < 0.0001).
Apart from gestation (< 28/40) and birth weight (< 1 kg), the following risk factors displayed a statistically significant corelation with ROP positive patients (Table 1). Hypoxia at birth, duration of oxygen supplementation, chronic lung disease (defined as oxygen dependency in premature babies at/beyond 36 weeks corrected gestational age), intra-ventricular haemorrhage, thrombocytopenia, anaemia, late onset sepsis, hypotension, patent ductus arteriosus and use of total parenteral nutrition (p<0.05). Various factors with no statistically significant correlation included gender, multiple pregnancies, Respiratory Distress Syndrome (RDS), hypothermia and hypoglycaemia on admission to neonatal unit.
Table 1: Risk factors and their statistical significance correlation with ROP.
ROP +ve |
ROP –ve |
P Value |
Odds Ratio (95% CI) |
|
Anaemia |
14 (82.4%) |
44 (24.2%) |
<0.0001 |
14.63 (4.02-53.29) |
Birth weight < 1 kg |
15 (88.2%) |
20 (11.0%) |
<0.0001 |
60.75 (12.93-285.3) |
Chronic lung disease |
16 (94.1%) |
34 (18.7%) |
<0.0001 |
69.64 (8.93-543.4) |
Duration of Oxygen therapy in days (mean) |
91 (75-106) |
19 (15-23) |
<0.0001 |
|
Gender |
Males = 10 (58.8%) |
Males = 108 (59.3%) |
1 |
0.9788 (0.356-2.688) |
Gestation < 28/40 |
15 (88.2%) |
25 (13.7%) |
<0.0001 |
47.1 (10.15-218.5) |
Hypoglycaemia on admission |
2 (11.8%) |
37 (20.3%) |
0.53 |
0.5225 (0.114-2.39) |
Hypotension |
6 (35.3%) |
11 (6.0%) |
0.0011 |
8.48 (2.64-27.23) |
Hypothermia on admission |
5 (29.4%) |
57 (31.3%) |
1 |
0.9137 (0.307-2.716) |
Hypoxia at birth |
16 (94.1%) |
105 (57.7%) |
0.0031 |
11.73 (1.52-90.38) |
Intraventricular haemorrhage |
10 (58.8%) |
35 (19.2%) |
0.00079 |
6.0 (2.13 – 16.87) |
Late onset neonatal sepsis (including NEC) |
13 (76.5%) |
36 (19.8%) |
<0.0001 |
13.2 (4.06-42.8) |
Multiple pregnancies (twins) |
3 (17.6%) |
46 (25.3%) |
0.57 |
0.634 (0.174-2.304) |
Patent ductus arteriosus |
12 (70.6%) |
25 (13.73%) |
<0.0001 |
15.07 (4.89-46.4) |
Respiratory distress syndrome |
15 (88.2%) |
121 (66.5%) |
0.099 |
3.78 (0.84-17.1) |
Thrombocytopenia |
6 (35.3%) |
15 (8.2%) |
0.0039 |
6.07 (1.97-18.7) |
Total parenteral nutrition |
15 (88.2%) |
85 (46.7%) |
0.0015 |
8.56 (1.90-38.5) |
Odds ratios and confidence intervals calculated using http://vassarstats.net |
||||
Logistic Regression
Stepwise logistic regression was carried out using raw data to identify a predictive algorithm for ROP: (https://stats.blue/Stats_ Suite/multiple_linear_regression_calculator.html). Categorical data was designated using 1 = condition present, 0 = condition absent. Gestation and birth weight were tested untransformed and after log transformation. Log transformation was found to be more effective. With each iteration of the calculator the least significant parameter was removed. Eventually after removing non-significant data (i.e. P>0.05) the only two variables remaining were gestation and birthweight. Birthweight was also found to be non-significant. However, since gestation and birthweight are correlated variables a standardised birthweight was calculated. Two methods of standardisation were tested – Multiple of the Median (MoM) (as used in antenatal Down’s screening (REF A)) and a Z score [7]. These were generated by regressing birthweight against gestation. MoMs were found to be better than Z-scores but despite this, when Loge (Birthweight MoM) was used in the logistic regression, the birthweight remained non-significant (P=0.0821). The best predictive algorithm therefore simply included gestation:
P(ROP) = ______________1_________________
1_ e-(108.333 – 33.4253 x LOGe(Gest(wks)))
A Receiver-Operator Curve for the predictive algorithm is shown in Figure 2. The P value cut offs for the first 4 data points are 0.995, 0.981, 0.936 and 0.812 respectively. Unfortunately, the data set is too small to allow boot-strapping analysis, so will clearly be over-optimistic in real life because the algorithm has been tested against the dataset upon which it was based. It would be helpful if other researchers could compare their data against this algorithm.
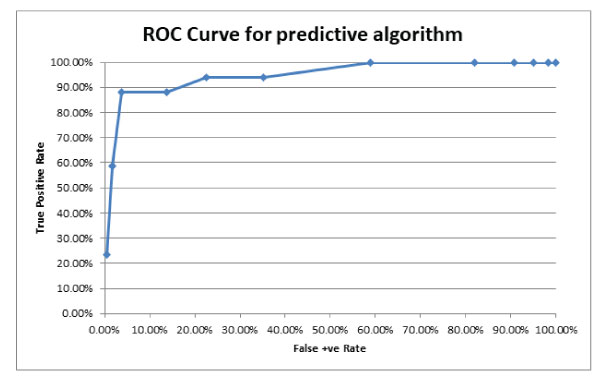
Figure 2: Receiver Operator curve showing predictive value of the logistic algorithm.
Similar to our results, in comparable studies from across the world, researchers have universally found statistically significant correlation between ROP and extreme prematurity as well as very low birth weight [8]. In other studies, the incidence of ROP has been found to be similar in Caucasian as well as Black babies, although the occurrence of threshold ROP was found to be higher in the Caucasian infants [9]. Because of relatively smaller sample size, we didn’t look at the incidence of ROP in various ethnic groups in our cohort. In our study, we found no significant correlation between multiple pregnancies and ROP. However, researchers from Singapore reported statistically significant difference between the two [10]. Nevertheless, this may well be a potential confounding factor as multiple pregnancies are at higher risk to premature delivery and low birth weight. Most of the studies report no correlation between ROP and gender or RDS. A contrasting observation has been published by Hakeem AHAA and colleagues who concluded that there is no correlation between ROP and gender, type of delivery, birth weight, patent ductus arteriosus, intra-ventricular haemorrhage, hypotension or duration of oxygen therapy [11].
Given what is known about ROP, it may appear surprising that duration of oxygen therapy was not found to be significant in the logistic regression, especially since there was a statistically significant difference between the duration in the two groups. The problem is that whilst statistically the ROP patients had a longer duration of therapy, logistic regression looks for predictive ability and there were sufficient babies without ROP but with a long duration of therapy, meaning that there was no predictive information in the data. It may be that an integral variable composed of percentage O received and duration (similar to the integral used for evaluating cigarette usage (pack years) could have greater significance but there was insufficient data available to allow assessment of total O2 load received to be assessed. Careful monitoring of oxygen administration and oxygen saturation is crucial part of preterm neonatal care. Wide fluctuations in oxygen saturations along with high O2 saturations soon after birth and for the first several weeks of age is associated with a higher incidence of severe ROP, greater need of laser treatment, higher incidence of blindness and CLD [12].
Neonatal hypotension, in addition to prematurity and low birth weight, was listed among the significant risk factors for ROP on a recently published meta-analysis [13]. This matches the outcomes from our local study which showed statistically significance correlation between them (Table 1). This metaanalysis also concluded that chorioamnionitis, prolonged rupture of membrane and induced fertility also increased the risk of developing ROP [13]. Researchers from Iran conducted a similar study with comparable sample size to our study. They found relatively higher incidence of ROP (33.3%) compared to our study (8.5%). They also identified that blood transfusion, birth weight and gestational age were independent ROP risk factors [14]. In contrast to most of the studies, the Brazilian researchers studied the risk factors in heavier and relatively late preterm infants (birth weight > 1500 g or gestational age between 32 to 37 weeks) [5]. In this retrospective Cohort study, they found that only a negligible number of infants born at >32 weeks gestation or with birth weight >1500g developed ROP, all of which had Stage 1 ROP which did not require treatment. These results are reassuring for most of the countries including United Kingdom who limit their ROP screening protocols to babies born at < 32/40 gestation and/ or birth weight < 1501 gms [2,3].
The main strength of our study is our ability to use the National neonatal computer system database (Badgernet) that helped to identify every eligible baby within the study period in a quick and timely fashion. Hospital electronic records were also used to cross checks the data and to collect additional information. Limitations of our study include relatively smaller sample size and difficulty in obtaining comprehensive data for babies who were transferred to regional units within the UK.
In summary, this study highlights a number of risk factors that contribute to increased risk of developing ROP many of which have consistently illustrated correlation over time and in different parts of the world. Our study also confirmed that gestational age and birth weight are among the agreed independent risk factors, in addition to strong correlation with some other risk factors as outlined in Tables 1.
Authors’ Contribution
Project Design, Data analysis, Literature search, Manuscript: RE, MA
Supervision, Manuscript review and approval/submission: MA
Data collection, Manuscript: RE, SJ, KB
Data analysis, Manuscript: SJ, NM, TM, KB, TR
Acknowledgement
We are grateful to the audit department at University Hospitals of Derby and Burton NHS Foundation Trust for allowing us to carry out this service evaluation project.
Conflicts of interest
We declare no conflict of interests.
Financial Disclosure
There are no relevant financial or non-financial competing interests to report.