Introduction: The interruption of pregnancy reflects the lifestyles of a high rate of population under 29 years of age, as is the case in the State of Mexico, however, the policies of decriminalization of abortion that focus their interest on making reasoned, planned and systematic decisions of the woman, avoid the influence of friends, relatives and partner(s) at the time of carrying out the request for termination of pregnancy.
Material & methods: The objective of the present study was to establish the exploratory factorial structure of instruments that measured psychological–cultural variables around intentions and experiences related to the interruption of pregnancy. A non–experimental, exploratory and cross–sectional study was carried out with a non–probabilistic selection of 210 students. The adjustments of the theoretical relationships with respect to the weighted relationships were estimated using two structural models, one cultural and the other cognitive.
Results: The values factor explained 41% of the variance (alpha = 0.732). The belief factor explained 33% of the variance (alpha = 0.705). The perceptual factor explained 28% of the variance (alpha = 0.721). The motive factor explained 23% of the variance (alpha = 0.742). The attitudinal factor explained 17% of the variance (alpha = 0.701). The normative factor explained 14% of the variance (alpha = 0.758). The intentional factor explained 9% of the variance (alpha 0.784) and the experiential factor explained 7% of the variance (alpha = 0.791).
However, the fit and residual parameters ⌠χ2 = 356.46 (67df) p = 0.067; GFI = 0.990;
CFI = 0.975; RMSEA = 0.000⌡ of the structural model of dependency relationships between indicators and cultural factors evidenced the spurious incidence of perceptions about experiences of termination of pregnancy.
Keywords: Values; Beliefs; Perceptions; Motives; Attitudes; Norms; Intentions.
The interruption of pregnancy is one of the issues that causes and will continue to cause controversy due to the contrast between current realities and taboos fueled by the remnants of tradition and customs [1]. The fundamental one is the influence of the Catholic Church on collective behavior, especially by censoring a more open debate that allows generating and solving broader problems such as extreme poverty, violation of human rights in various ways [2]. To this, you can add the pregnancies that are generated from, for example, pregnancies resulting from rape [3]. Well, according to the Catholic Church, with the fertilization of the ovum, a life is inaugurated that is neither that of the father nor that of the mother, but that of a new human being that develops by itself.
The other leviathan that plagues the issue of the interruption of pregnancy is the criminalization of abortion, because due to a greater strength of the Catholic Church and a greater rootedness of the customs and traditions of the family and of society, it led to criminalize the interruption of pregnancy. pregnancy in some countries [4]. However, the criminalization of the interruption of pregnancy has not combated the high number of clandestine curettages, which often ends with irreversible damage and frequently the death of women. International organizations have dealt with this issue from different fronts. On the one hand, we find the international precepts and agreements that have been approved for the defense of life in its various manifestations, and on the other, we even find the same legislation that is concerned with the rights of women, especially the rights reproductive [5]. Situation that must be analyzed carefully, so as not to fall into contradictions in the legislation of each country.
In Mexico, the issue of abortion as a legal matter has a tradition of more than a century, because since the Penal Code of 1871, it had already been included as part of: "Crimes against persons, committed by individuals" [6]. This structure was maintained over the years, going through the Codes of 1929, 1931. Perhaps the most recent novelty in terms of the interruption of pregnancy, is the reform that was made in the government of the Federal District in 2007 to the Penal Code for the Federal District [7]. Well, somehow, it meant the beginning of the decriminalization of abortion through the legal interruption of pregnancy before the twelfth week of gestation.
With the previous reform, the interruption of pregnancy in recent years has become a public problem [8]. With this, the private and public space have been confronted, fundamentally, because it is about the decision of women on a public issue fed by social groups such as religion or family, regulated under legal elements that have been established by the State [9]. This is precisely what makes up a thorny field of study, since a fair mean of the different actors leaves all the actors unsatisfied, since the definition of the interruption of pregnancy as a public problem is not necessarily religious, ethical or legal.
However, it is essential to investigate its constitution process, since it can be raised from general issues such as human reproduction, the exercise of sexuality, human freedom, public health or the right to life [10]. But it can also be constituted from some more specific issues such as problems during pregnancy, cases of rape, due to health risks for women, non–consensual artificial insemination, imprudent abortion, due to genetic malformations, due to lack of resources of the parents, among others [11]. To be inserted in this discussion, it is essential to have knowledge about a conceptual framework, both medical and legal, that establishes the field of abortion [12]. Among them, we find the topic of conception, fertilization, pregnancy, abortion, legal abortion.
The multiple edges and positions from which it is analyzed give rise to controversies due to moral, ethical, legal and religious conflicts [13]. Regardless of the position, it is essential to recognize that it is part of our social reality, whether it is legally acceptable or not [14]. From the controversies, knowledge is little and institutional recognition is even more so [15]. Knowledge of abortion has been slow and gradual in Mexican society, since it is considered illegal, there is no institutional way to establish a registry [16]. Well, the National Institute of Statistics and Geography (INEGI), only keeps records when this is considered a crime [17]. The efforts of civil society are insufficient to maintain the registry, even more so when it comes to clandestine abortions.
In the arena of the dispute, in which abortion is defined as a public problem, each of the “interested” actors tries to establish a public agenda based on their positions and interests [18]. However, the actors in the process of defining the problem do not necessarily reflect the social representations that the various sectors of the population have, especially since there is a multiplicity of mixtures of social scenarios.
Studies of the request for induced abortion or termination of pregnancy warn of three determining factors; a) socioeconomic, since as poverty intensifies, sexuality increases, unwanted pregnancies increase and clandestine abortion practices are exacerbated; b) religious as inhibitors of sexuality and once an unwanted pregnancy occurs, abortion; c) normative–values in which the family and groups close to requesters of termination of pregnancy influence the decision.
The medical literature on abortion warns of a propensity for abortion practice based on beliefs, attitudes and knowledge of both patients and doctors [19]. It is a cultural system in which the knowledge of health professionals is influenced by their beliefs and attitudes. In this way, the actors; health professionals, patients and family members, constitute a system of adherence or repulsion to the interruption of pregnancy.
In the case of studies with couples, abortion depends on the type of relationship [20]. If it is significant, then the decision to request an abortion is negotiated, consensual and co–responsible [21]. If the relationship is short–lived and without any commitment, then the decision is made by the parents of the couple [22]. In other words, the determinants of abortion are based on a cultural system of values, norms, and beliefs that explain the mediation of attitudes and intentions in the request for termination of pregnancy.
The literature has established the dependency relationships between psychological–cultural variables such as norms, values, perceptions and experiences [23]. The established model includes three hypotheses in which values are the determining factor of experiences, but also this factor of moral and ethical principles that guide behavior affects the experiences of pregnancy termination through norms and perceptions [24]. The model explains those cases in which social values, disseminated in local uses and customs, as well as in parenting, friendship and courtship styles, directly and indirectly affect the experiences of pregnancy interruption.
In contrast, the specification of a model of cognitive dependency relationships would explain decision–making around pregnancy termination as the result of deliberate, planned and systematic information processing (beliefs) that would be mediated by dispositions in favor of termination of pregnancy. termination of pregnancy (attitudes) and the reasons (motives) for carrying out an intentional abortion [25]. Therefore, the establishment of the factorial structure of both models of dependency relationships between indicators and psychological–cultural factors will allow the contrast of both models with the purpose of influencing reproductive health policies in community health centers.
What are the psychological dimensions surrounding the request for termination of pregnancy?
Theoretical psychological dimensions—values, beliefs, perceptions, motives, attitudes, norms, intentions, and experiences—fit the weighted dimensions [26]. Theoretical psychological dimensions are different from the weighted dimensions.
Design
A correlational and cross–sectional study was carried out.
Sample
A non–probabilistic selection of 100 students from a public university in Huehuetoca, State of Mexico, was carried out. 45% are men and 65% are women; with a mean age (M = 19.21, SD = 0.81) and income (M = 718 USD, SD = 1.92 USD).
Sample
Scales of Variables related to the Interruption of Pregnancy (Table 1).
Table 1: Variables operationalization.
Variable |
Definition |
Scale |
Value |
It includes seven items around the principles that guide the decision to terminate the pregnancy |
0 = “it is not at all like my situation” to 5 = “it is very similar to my situation” |
Beliefs |
It includes seven questions about the processing of information related to the interruption of pregnancy |
0 = “false” and 1 = “true” |
Perception |
It includes seven items regarding expectations when requesting the termination of pregnancy |
0 = “not at all likely” to 5 = “very likely” |
Motive |
It includes seven questions about the reasons for requesting a termination of pregnancy |
0 = “not at all like my situation” to 5 = “very similar to my situation” |
Attitude |
It includes seven items regarding the provisions for requesting the termination of pregnancy |
0 = “not at all in agreement” to 5 = “strongly in agreement” |
Norms |
It includes seven reagents about uses and customs related to the interruption of pregnancy |
0 = "nothing similar to my situation" to 5 = "very similar to my situation". |
Intention |
It includes seven items on decision–making related to pregnancy termination |
0 = “not at all likely” to 5 = “very likely”. |
Experiences |
It includes seven items around actions aimed at the termination of pregnancy |
0 = "I have not had that experience" and 1 = "I have had that experience". |
Source: Elaborated with literature review |
||
Sample
Preliminary interviews were conducted to explore norms, values, perceptions, beliefs, attitudes, motives, intentions, and actions around the request for induced abortion. Once the conceptual dimensions were established, the items were constructed. Subsequently, it was massively applied, and the items were excluded. Once the scales were established, their final application was carried out. At the time of handing in the questionnaires, they were informed that their responses would not have an indirect or direct, negative or positive impact on their grades. Subsequently, the data was processed in the Statistical Package for Social Sciences (SPSS) and Analysis of Structural Moments (AMOS).
Analysis
Dependency relationships were established between each of the variables following the established hypotheses. Once a significant relationship between each of the variables was verified, the model and its adjustment with indices and residuals were estimated.
Normality
The normal distribution was estimated with the multivariable kurtosis parameter assuming that a value less than five is evidence of normality and the Bootstrap sampling and significance statistic with a value close to zero.
Reliability
Internal consistency was estimated with the subscale item correlation for which an alpha value greater than 0.60 and less than 0.90 was assumed as evidence of reliability. Items that lowered the required threshold were discarded.
Validity
The Kayser Meyer Olkin (KMO) parameters and the Bartlet test were weighted to establish adequacy and sphericity, while the factor–item correlation from an Exploratory Factor Analysis of principal axes with promax rotation and obliquity criteria was considered as evidence of construct validity if the value is greater than 0.300.
Structure
An exploratory factor analysis was carried out, considering values below 0.90 and above 0.40 as evidence of a dependent relationship, while values close to zero were assumed to be spurious relationships. In contrast, values greater than 0.90 were considered as evidence of collinearity and multicollinearity.
Adjust
The hypothesis contrast was performed with the chi square statistic whose value and level of significance close to zero were assumed as evidence of acceptance of the null hypothesis [27]. On the contrary, values greater than 0.05 were considered as evidence of acceptance of the alternative hypothesis. However, since the sample consisted of 210 students, the chi–square parameter turned out to be sensitive to the size of the sample. This is how the Goodness of Fit Index (GFI) and the Mean Square Error of Approximation (RMSEA) were included.
Table 2 shows the normal distribution, reliability and validity required for the contrast of the model of relationships specified in seven hypotheses. That is, the kurtosis values indicate the distribution of the responses of the respondents in such a way that it allows inferring the consistency of these same results in other samples or latitudes in which the eight factors will emerge forming a structure of dependency relationships. Precisely, the empirical test of these hypotheses is presented below.
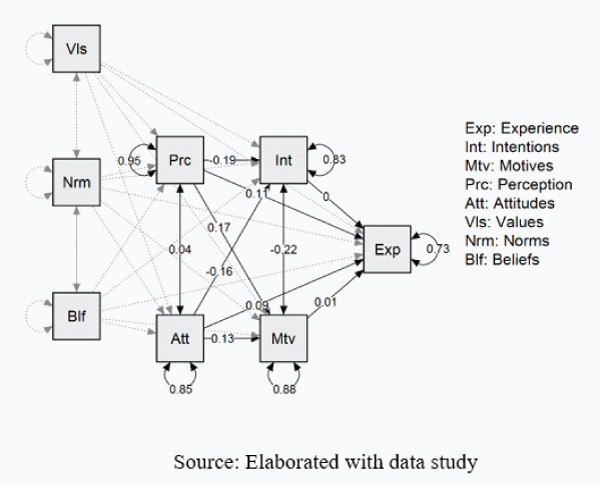
The experiences related to the termination of pregnancy were determined by the expectations surrounding the request for assisted abortion, although these perceptions were determined to a lesser extent by the values. In other words, the values seem to reduce the influence of a psychological factor such as perception in relation to the experience of requesting an induced abortion (Figure 1).
The fit and residual parameters ⌠χ2 = 356.46 (67df) p = 0.067; GFI = 0.990; CFI = 0.975; RMSEA = 0.000⌡ show the acceptance of the null hypothesis regarding the adjustment of the theoretical psychological–cultural relationships with respect to the estimated relationships.
Table 2: Descriptive of the instrument.
M |
SD |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
r1 |
3.01 |
0.82 |
||||||||
r2 |
2.93 |
0.73 |
0.712 |
|||||||
r3 |
2.81 |
0.71 |
0.415 |
|||||||
r4 |
2.71 |
0.82 |
0.832 |
|||||||
r5 |
3.71 |
0.39 |
0.713 |
|||||||
r6 |
2.71 |
0.46 |
||||||||
r7 |
2.81 |
0.31 |
||||||||
r8 |
1.71 |
0.37 |
||||||||
r9 |
1.27 |
0.36 |
||||||||
r10 |
1.39 |
0.82 |
0.68 |
|||||||
r11 |
1.01 |
0.81 |
0.491 |
|||||||
r12 |
1.72 |
0.93 |
||||||||
r13 |
1.42 |
0.49 |
||||||||
r14 |
1.57 |
0.57 |
0.824 |
|||||||
r15 |
3.81 |
0.71 |
||||||||
r16 |
2.31 |
0.29 |
||||||||
r17 |
1.82 |
0.49 |
||||||||
r18 |
3.49 |
0.57 |
0.491 |
|||||||
r19 |
2.37 |
0.72 |
0.284 |
|||||||
r20 |
2.81 |
0.61 |
||||||||
r21 |
1.8 |
0.83 |
||||||||
r22 |
1.92 |
0.71 |
||||||||
r23 |
3.14 |
0.87 |
0.491 |
|||||||
r24 |
2.93 |
0.77 |
0.592 |
|||||||
r25 |
1.64 |
0.73 |
||||||||
r26 |
2.15 |
0.28 |
0.492 |
|||||||
r27 |
1.03 |
0.49 |
||||||||
r28 |
1.46 |
0.75 |
||||||||
r29 |
3.13 |
0.93 |
||||||||
r30 |
3.54 |
0.72 |
||||||||
r31 |
2.57 |
0.49 |
||||||||
r32 |
3.59 |
0.39 |
0.491 |
|||||||
r33 |
3.81 |
0.61 |
||||||||
r34 |
1.5 |
0.49 |
0.713 |
|||||||
r35 |
2.8 |
0.28 |
||||||||
r36 |
2.91 |
0.84 |
||||||||
r37 |
1.93 |
0.69 |
||||||||
r38 |
1.82 |
0.58 |
||||||||
r39 |
2.67 |
0.64 |
||||||||
r40 |
3.81 |
0.55 |
0.629 |
|||||||
r41 |
2.94 |
0.38 |
–0.827 |
|||||||
r42 |
1.04 |
0.58 |
||||||||
r43 |
1.21 |
0.59 |
||||||||
r44 |
1.04 |
0.73 |
–0.412 |
|||||||
r45 |
1.05 |
0.59 |
||||||||
r46 |
1.04 |
0.49 |
0.719 |
|||||||
r47 |
1.06 |
0.29 |
||||||||
r48 |
1.09 |
0.49 |
||||||||
r49 |
1.82 |
0.39 |
||||||||
r50 |
1.04 |
0.42 |
||||||||
r51 |
1.05 |
0.84 |
738 |
|||||||
r52 |
1.16 |
0.34 |
||||||||
r53 |
1.52 |
0.49 |
0.826 |
|||||||
r54 |
1.27 |
0.58 |
0.476 |
|||||||
r55 |
1.26 |
0.28 |
0.604 |
|||||||
r56 |
1.03 |
0.48 |
||||||||
Extraction method: Main axes with promax rotation and obliquity criterion. Multivariate Kurtosis = 2.394; KMO=0.719; X 2 = 3.719, 15df, p = 0.000, F1 = Values (41% of the total variance explained), F2 = Beliefs (33% of the total variance explained), F3 = Perceptions (28% of the total variance explained), F4 = Motives (23% of the total variance explained), F5 = Attitudes (17% of the total variance explained), F6 = Norms (14% of the total variance explained), F7 = Intentions (9% of the total variance explained ); F8 = Experiences (7% of the total variance explained). M = Mean, SD = Standard deviation, C = Kurtosis |
||||||||||
The contribution of this study to the state of knowledge and the literature consulted lies in the establishment of an exploratory factorial structure of dependency relationships between indicators and psychological–cultural factors as determinants of intentions and experiences related to the interruption of pregnancy.
However, the findings of this research:
The contribution of this work to the state of the question lies in the establishment of a trajectory model in which the measurement of cognitive factors determines the relationship between sociocultural and behavioral factors. In this way, lines of studies related to the mediation of sociocultural and sociocognitive factors in the relationship between environmental factors such as insecurity about the request for interruption of pregnancy. Public policies and the local agenda can benefit from the established findings. Crime prevention strategies and programs can be defined based on the findings related to the determinants of the experiences of pregnancy interruption.
None.
Author declares there is no conflict of interest.