Ocular infections have been associated with bacterial contamination of eyeglasses. This study assessed bacterial contaminants associated with the eyeglasses of staffs and students of Babcock University, Ilishan–Remo, Ogun State, Nigeria. A total of 100 participants comprising 33 males and 67 females (aged 16–76 years) were recruited for the study after obtained their written informed consents. Ethical approval for the study was obtained from the Babcock University Health Research Ethics Committee (Ethical registration number: BUHREC484/18). A structured questionnaire was used to gather the participants’ demographic and clinical information. A total of 100 eyeglasses were examined for bacterial contamination using standard bacteriological methods. A one–way analysis of variance (ANOVA) and Turkey–Kramer Multiple Comparisons Test were performed using Statistical Package for Social Sciences version–18 (SPSS–18.0) software to determine the differences between the bacterial loads among the eyeglasses of study participants. The percentage of eyeglass lenses with unacceptable levels of contamination (>105CFU/mL) (19%) was significantly lower (P<0.05) than those with acceptable levels of contamination (<104CFU/mL) (46%). While, the percentage of eyeglass handles with unacceptable level of contamination (49%) was significantly higher (P<0.05) than those with acceptable levels of contamination (7%). Most of the isolated bacterial were sensitive to the antibiotics tested. Risk factors associated with bacterial contamination of eyeglasses include: exposure to dusty environment, irregular cleaning and poor compliance with eyeglass care guidelines. The outcome of this study further underscore the claim that eyes glasses may serve as potential vehicles for bacteria capable of causing ocular infections.
Keywords: Antibiotic Susceptibility; Bacterial pathogen; Contamination; Eye glasses; Risk factors.
Ocular infections are common [1, 2] and have been associated with microbial contamination of contact lenses and eyeglasses [3,4]. Daily, whether in the market, schools, churches, the comfort of our homes, or even in our offices, we are unknowingly exposed to many pathogens [5]. Unfortunately, many frequently used devices, such as eyeglasses and contact lenses, are rarely sterilized or kept clean, which increases the likelihood of bacterial contamination and colonization [6,7].
Various people today wear eyeglasses (spectacles) for functional or purely cosmetic reasons [8,9]. The human eye has a special anatomy that makes it vulnerable to several infectious agents, including bacteria, as well as direct environmental exposure. The eyelid, conjunctiva, and cornea are the main parts of the eye that are most frequently infected. Several ocular illnesses, including conjunctivitis, keratitis, scleritis, choroiditis, iridocyclitis, retinal vasculitis, retinitis, and posterior uveitis, have been linked to contamination of handles and lenses of eyeglasses. This is quite worrisome, because these bacteria are transferred to the eyewear through contact with infected hands and other methods [3].
Numerous microorganisms have been linked to eye infections caused by microbial contamination and colonization of eyeglasses. While Butt et al. [4] reported the presence of bacterial contaminants such as Staphylococcus species, Streptococcus species, Pseudomonas species, Aeromonas species, Citrobacter species, Haemophilus influenza, Chlamydia trachomatis and Neisseria gonorrhoeae on Surgeon’s eyeglasses; Nwaugo et al. [8] reported the presence of fungal contaminants such as Microsporium species, Penicillium species, Aspergillus species, Trichophyton species and Candida species on the eyeglasses of patients attending ophthalmology clinic at Abia State University, Uturu, Nigeria. In his paper titled "Eyewear contamination levels in the operating room: Infection risk," Lange [10] named reported three species as potentially implicated agents: Enterococcus species, Staphylococcus species, and Aspergillus species. Still, Osaro–Matthew et al. [11], reported the presence of Klebsiella species (1.89%), coagulase negative staphylococcus (9.43%), Bacillus species (13.21%), Pseudomonas aeruginosa (13.21%), Streptococcus species (16.98%), Staphylococcus aureus (28.30%) and Escherichia coli (51.89%) on the medicated eye glasses worn by Students and Staff of a public tertiary institution in south–east, Nigeria.
It is yet unknown how eyeglass lenses and frames increase the risk of ocular infection. However, the most likely explanation is that throughout any given day, our hands come into contact with an endless variety of items and surfaces. We can easily transfer any bacteria, mold, or irritating residues from our hands to our glasses while handling, putting on, or taking off the glasses. The cycle then continues as the bacteria grow on our glasses and finally find their way to our eyes.To the best of our knowledge, there is no information available on the quantity, frequency, and distribution of bacterial contamination found on Babcock University personnel and students' eyeglasses in Ilishan–Remo, Ogun State. This research is necessary due to the dearth of data in this area. The aim of this study is therefore to assess the load, frequency and distribution of bacterial contaminants present on the eye glasses used by staff and students of Babcock University, Ilishan–Remo, Ogun State. The study intended to evaluate the antibiotic sensitivity pattern of the recovered bacterial isolates in addition to trying to discover risk variables linked to bacterial contamination of participants’ eyeglasses.
Study area
This study was conducted at Babcock University, a premier Seventh–day Adventist institution of higher learning situated in the South–Western area of Nigeria, in Ilishan–Remo, Ikenne Local Government Area, Ogun State, coordinates: 6.8862o N, 3.7055o E (https://goo.gl/maps/kcxoqg9iakBFWriX6).
Study design, population and sample size
<This cross–sectional descriptive study lasted for three months (April–June, 2018), The targeted audience were Babcock University students and faculty (aged 16 and older) who wear glasses, whether functional or cosmetic, regardless of their tribal, religious, and cultural affiliations.
The population proportion formula described by Charan and Biswas [12] was used to estimate the sample size (n) required for the study:
n = Z2PQ/d2
Where;
n = required sample size,
Z = Standard normal variate at 5% (p<0.05) error or 95% confidence interval is 1.96
P = Proportion of eyeglasses with bacterial contaminants from previous study,
Q = Proportion of eyeglasses without bacterial contaminants (1 – P) and
d = Absolute error margin is 0.05
The minimal sample size needed was calculated using a 95% confidence interval, a p value of 0.934, or a prevalence rate of 93.4% from a prior study by Osaro–Matthew et al. [11], and a margin of error (d) set at 0.05. A final sample size of 100 was obtained by adding 5% of the original sample size in order to reduce mistakes caused by the possibility of non–compliance.
Sampling and data collection
Simple random sampling was used to choose the study subjects from among the University's nine schools. Through the distribution of structured questionnaires to the participants, demographic and medical information on the participants was gathered. The participants' biographical information, including occupation, gender, marital status, age, and tribe, was included in the first section of the questionnaires. Data on different types of eyeglasses, how to care for and maintain them, history of past eye infections, risk factors, personal hygiene, and health care seeking behavior were all included in the second section.
Specimen collection, transportation and laboratory analysis
Each participant's eyeglass lenses and handles were swabbed with two different sterile cotton tipped applicators that had been soaked with sterile peptone water (Panreac–AppliChem, Spain) using proper aseptic methods. Each swab stick was severed at the hank region, and the head holding the cotton was aseptically put into a sterile bottle containing ten millilitres (10 mL) of peptone broth. The bottle was then promptly corked properly using aseptic techniques (including wearing of sterile hand gloves). The samples were then brought to the laboratory in a tightly sealed case and processed there within eighteen hours (18 hr) of being collected from the personnel and students.
Determination of Bacterial Count
The contents of the bottles were allowed to stay for thirty minutes (30 min) before being vortexed for sixty seconds. Ten–fold serial dilutions was thereafter prepared using sterile distilled water and 0.02ml of appropriate dilution was spread onto sterile Nutrient agar, Blood agar and MacConkey’s agar, contained in petri–dishes with 0.05mg/ml of Ketoconazole added to inhibit fungal growth. The surface viable count as described by Miles and Misra [13] was used for the determination of bacterial load in the eye glass swabs. The number of colony forming units (CFU) per mL from the original eye glass swab broth sample was calculated using the given equation: CFU/ml = Mean no of colonies x no of drops/ml x dilution factor. The petri dishes were then incubated aerobically at 370C for twenty four hours. Colonies from the plates thereafter were purified and stored on nutrient agar slants for characterization and identification.
Isolation of Pure Cultures
Purity plate was done for mixed cultures using the streak plate technique as described by Ochei and Kolhatkar [14]. Aseptic streaking of the inoculum with the aid a wire loop resulted in continuous dilution of the inoculum to give well separated distinct colonies.
Identification of Bacterial Isolates
After incubation, plates containing cultured samples were examined and colonies of bacteria were identified Gram–stained. Gram negative bacteria were identified further by biochemical tests such as motility, oxidase, sugar fermentation, urea hydrolysis, indole, citrate, hydrogen sulfide, methyl red and Voges–Proskauer tests, while, Gram positive cocci were characterized by performing catalase and coagulase test as described by Cheesbrough [15]. The results of theses tests were entered into IDENTAX bacterial identifier (Sun Microsystems’s Java Technology) for the taxonomical identification of bacteria isolates on the basis of their phenotypical characteristics. Pure cultures of the identified organisms were stored on Nutrient agar slant for subsequent antibiotic sensitivity testing.
Determination of the antibiotic sensitivity pattern of bacterial isolates
The antibiotic sensitivity pattern of the bacterial isolates was determined using the disc diffusion technique as described by Bauer et al. [16] and Cheesbrough [17]. Using the Interpretative chart, the zone of inhibition of each antibiotic was interpreted as ‘Resistant’, ‘Intermediate/, or ‘Susceptible’.
Data analysis
A one–way analysis of variance (ANOVA) and Turkey–Kramer Multiple Comparisons Test were performed using Statistical Package for Social Sciences version–18 (SPSS–18.0) software to determine the differences between the bacterial loads among the eyeglasses of study participants. P values<0.05 was considered significant.
The demographic characteristics of the participants are presented in Table 1. A total of 100 participants comprising 33 males and 67 females were recruited for the study. Majority of the participants belong to the age group 16–25 years (36%), while the least belong to 76 years and above (2%). Based on their marital status, 76% were single, while 24% were married. With regard to their occupation, 24% were Staff, while 76% were Students. On the account of religion, majority of the participants were Christians (76%) while the least were Muslims (24%). Based on tribe, most of them were Yoruba (42%) while the least were Hausa (3%).
Table 1: Demographic characteristics of the study participants.
Characteristics |
Category |
Number (N) |
Percentage (%) |
Sex |
Male |
33 |
33 |
Female |
67 |
67 |
|
Age group (Years) |
16–25 |
36 |
36 |
26–35 |
20 |
20 |
|
36–45 |
16 |
16 |
|
46–55 |
11 |
11 |
|
56–65 |
10 |
10 |
|
66–75 |
5 |
5 |
|
76 and above |
2 |
2 |
|
Marital status |
Single |
76 |
76 |
Married |
24 |
24 |
|
Occupation |
Staff |
24 |
24 |
Student |
76 |
76 |
|
Religion |
Christianity |
76 |
76 |
Islam |
24 |
24 |
|
Traditional |
0 |
0 |
|
Tribe |
Yoruba |
42 |
42 |
Ibo |
25 |
25 |
|
Hausa |
3 |
3 |
|
Others |
30 |
30 |
Table 2: Frequency of bacterial contamination of lenses and handles of eye glasses according to the demographic characteristics of the study participants.
Characteristics |
Category |
Number examined N (%) |
Number of Lenses contaminated N (%) |
Number of Handles contaminated N (%) |
P–value |
Sex |
Male |
33 (33) |
33 (33) |
33 (33) |
0.711 |
Female |
67 (67) |
67 (67) |
67 (67) |
0.313 |
|
Age group (Years) |
16–25 |
36 (36) |
36 (36) |
36 (36) |
0.223 |
26–35 |
20 (20) |
20 (20) |
20 (20) |
0.359 |
|
36–45 |
16 (16) |
16 (16) |
16 (16) |
0.354 |
|
46–55 |
11 (11) |
11 (11) |
11 (11) |
0.362 |
|
56–65 |
10 (10) |
10 (10) |
10 (10) |
0.302 |
|
66–75 |
5 (5) |
5 (5) |
5 (5) |
0.362 |
|
76 and above |
2 (2) |
2 (2) |
2 (2) |
0.365 |
|
Marital status |
Single |
76 (76) |
76 (76) |
76 (76) |
0.88 |
Married |
24 (24) |
24 (24) |
24 (24) |
0.757 |
|
Occupation |
Staff |
24 (24) |
24 (24) |
24 (24) |
0.88 |
Student |
76 (76) |
76 (76) |
76 (76) |
0.757 |
|
Religion |
Christianity |
76 (76) |
76 (76) |
76 (76) |
0.28 |
Islam |
24 (24) |
24 (24) |
24 (24) |
0.242 |
|
Traditional |
0 (0) |
0 (0) |
0 (0) |
||
Tribe |
Yoruba |
42 (42) |
42 (42) |
42 (42) |
0.43 |
Ibo |
25 (25) |
25 (25) |
25 (25) |
0.153 |
|
Hausa |
3 (3) |
3 (3) |
3 (3) |
0.234 |
|
Others |
30 (30) |
30 (30) |
30 (30) |
0.325 |
|
P value >0.05 is considered statistically not significant. |
|||||
Furthermore, the bacterial load on the eye glass lenses of the participants according to their demographic characteristics is presented on Table 3. Forty six (46%) of the lenses examined had bacterial load below <104CFU/mL (Acceptable level of contamination), 35% falls between 104–105 CFU/mL (Inconclusive), while 19% had bacterial load above 105 CFU/mL (Unacceptable level of contamination). The percentage of eyeglass lenses with unacceptable level of contamination was higher than those with acceptable level of contamination. Meanwhile, there was no significant difference (P>0.05) in the level of contamination between and within the categories of participants.
Table 3: Bacterial load on the lenses of eye glasses of the participants according to their demographic characteristics.
Demographic Characteristics |
Category |
Bacterial Load |
|||
<104 CFU/mL N (%) |
104–105 CFU/mL N (%) |
>105 CFU/mL N (%) |
P–value |
||
Sex |
Male |
15 (45.5) |
11 (33.3) |
7 (21.2) |
0.919 |
Female |
31 (46.3) |
24 (35.8) |
12 (17.9) |
||
Total |
46 (46)* |
35 (35) |
19 (19) |
||
Age group (Years) |
16–25 |
19 (52.8) |
12 (33.3) |
5 (13.9) |
0.631 |
26–35 |
7 (35) |
8 (40) |
5 (25) |
0.567 |
|
36–45 |
9 (56.2) |
3 (18.8) |
4 (25) |
0.456 |
|
46–55 |
4 (36.4) |
4 (36.4) |
3 (27.3) |
0.651 |
|
56–65 |
4 (40) |
5 (50) |
1 (10) |
0.359 |
|
66–75 |
3 (60) |
1 (20) |
1 (20) |
0.368 |
|
76 and above |
0 (0) |
2 (100) |
0 (0) |
0.323 |
|
Total |
46 (46)* |
35 (35) |
19 (19) |
||
Marital status |
Single |
38 (50) |
25 (32.9) |
13 (17.1) |
0.35 |
Married |
8 (33.3) |
10 (41.7) |
6 (25) |
||
Total |
46 (46)* |
35 (35) |
19 (19) |
||
Occupation |
Staff |
8 (33.3) |
10 (41.7) |
6 (25) |
0.35 |
Student |
38 (50) |
25 (32.9) |
13 (17.1) |
||
Total |
46 (46)* |
35 (35) |
19 (19) |
||
Religion |
Christianity |
36 (47.4) |
29 (38.2) |
11 (14.5) |
0.108 |
Islam |
10 (41.7) |
6 (25) |
8 (33.3) |
0.12 |
|
Traditional |
0 (0) |
0 (0) |
0 (0) |
||
Total |
46(46.0)* |
35(35.0) |
19(19.0) |
||
Tribe |
Yoruba |
16 (38.1) |
14 (33.3) |
12 (28.6) |
0.624 |
Ibo |
10 (40) |
8 (32) |
7 (28) |
0.535 |
|
Hausa |
3 (100) |
0 (0) |
0 (0) |
0.658 |
|
Others |
17 (56.7) |
13 (43.3) |
0 (0) |
0.352 |
|
Total |
46 (46)* |
35 (35) |
19 (19) |
||
Key: Bacterial load < than 104CFU per mL = Acceptable level of contamination, Bacterial load between 104–105CFU per mL = inconclusive, Bacteria load >105 CFU per mL = unacceptable level of contamination. *Percentage of eyeglass lenses with acceptable level of contamination was significantly higher (P<0.05) in those with unacceptable level of contamination. Level of contamination between and within categories of participants is considered statistically not significant (P>0.05). |
|||||
Table 4 shows the bacterial load on the eyeglass handles of participants according to their demographic characteristics. 7% of them falls below 104CFU/mL (Acceptable level of contamination), 44% falls between 104–105CFU/mL (Inconclusive), while 49% falls above 105 CFU/mL (unacceptable level of contamination). The percentage of eyeglass handles with acceptable level of contamination was lower than those with unacceptable level of contamination. Meanwhile, there was no significant difference (P>0.05) in the level of contamination between and within the categories of participants.
Table 4: Bacterial load on the handles of eye glasses of the participants according to their demographic characteristics.
Demographic Characteristics |
Category |
Bacterial Load |
|||
<104 CFU/mL N (%) |
104–105 CFU/mL N (%) |
>105 CFU/mL N (%) |
P–value |
||
Sex |
Male |
3 (9.1) |
11 (33.3) |
19 (57.6) |
0.313 |
Female |
4 (6.0) |
33 (49.3) |
30 (44.8) |
||
Total |
7 (7) |
44 (44) |
49 (49) |
||
Age group (Years) |
16–25 |
1 (2.8) |
18 (50.0) |
17 (47.2) |
0.359 |
26–35 |
2 (10.0) |
6 (30.0) |
12 (60.0) |
0.567 |
|
36–45y |
2 (12.5) |
8 (50.0) |
6 (37.5) |
0.456 |
|
46–55 |
0 (0) |
3 (27.3) |
8 (72.7) |
0.651 |
|
56–65 |
2 (20.0) |
5 (50.0) |
3 (30.0) |
0.359 |
|
66–75 |
0 (0) |
2 (40.0) |
3 (60.0) |
0.368 |
|
76 and above |
0 (0) |
2 (100.0) |
0 (0) |
0.323 |
|
Total |
7 (7.0) |
44 (44.0) |
49 (49.0) |
||
Marital status |
Single |
5 (6.6) |
35 (46.1) |
36 (47.4) |
0.757 |
Married |
2 (8.3) |
9 (37.5) |
13 (54.2) |
||
Total |
7 (7.0) |
44 (44.0) |
49 (49.0) |
||
Occupation |
Staff |
2 (8.3) |
9 (9) |
13 (54.2) |
0.757 |
Student |
5 (6.6) |
35 (46.1) |
36 (47.4) |
||
Total |
7 (7.0) |
44 (44.0) |
49 (49.0) |
||
Religion |
Christianity |
5 (6.6) |
37 (48.7) |
34 (44.7) |
0.242 |
Islam |
2 (8,3) |
7 (29.2) |
15 (62.5) |
0.3 |
|
Traditional |
0 (0) |
0 (0) |
0 (0) |
||
Total |
7 (7) |
44 (44) |
49 (49) |
||
Tribe |
Yoruba |
3 (7.1) |
13 (31.0) |
26 (61.9) |
0.153 |
Ibo |
3 (12.0) |
10 (40.0) |
12 (48.0) |
0.146 |
|
Hausa |
0 (0) |
2 (66.7) |
1 (33.3) |
0.1 |
|
Others |
1 (3,3) |
19 (63.3) |
10 (33.3) |
0.213 |
|
Total |
7 (7) |
44 (44) |
49 (49) |
||
Key: Bacterial load < than 104CFU per mL = Acceptable level of contamination, Bacterial load between 104–105CFU per mL = inconclusive, Bacteria load >105 CFU per mL = unacceptable level of contamination. *Percentage of eyeglass handles with unacceptable level of contamination was significantly higher (P<0.05) than those with acceptable level of contamination. Level of contamination between and within categories of participants is considered statistically not significant (P>0.05). |
|||||
Table 5 shows the bacterial load on the eye glasses of the study participants according to the type of glasses and surface examined. In all, 150 medicated eyeglasses and 50 non–medicated eyeglasses were examined. There was no significant difference (P>0.05) between the proportion of medicated eyeglasses with acceptable level of contamination (25.4%) and those with unacceptable level (37.3%). Still, there was no significant difference (P>0.05) between the proportion of non–medicated eyeglasses with acceptable.
Table 5: Bacterial load on the eye glasses of the study participants according to the type and surface examined.
Type of eye glasses |
Surface examined |
Bacterial Load |
Total |
P–value |
||
<104 CFU/mL |
104–105 CFU/mL |
>105 CFU/mL |
||||
Recommended |
Lens |
32 (42.7) |
27 (36.0) |
16 (21.3) |
75 (37.5) |
0.434 |
Handles |
6 (85.7) |
29 (65.9) |
40 (81.6) |
75 (37.5) |
||
Total |
38 (25.4) |
56 (37.3) |
56 (37.3) |
150 (75) |
||
Non– recommended |
Lens |
14 (56.0) |
8 (32.0) |
3 (12.0) |
25 (12.5) |
0.172 |
Handles |
1(14.3) |
15(34.1) |
9 (18.4) |
25 (12.5) |
||
Total |
15 (30.0) |
23 (46.0) |
12 (24.0) |
50 (25.0) |
||
Key: Bacterial load < than 104CFU per mL = Acceptable level of contamination, Bacterial load between 104–105CFU per mL = inconclusive, Bacteria load >105 CFU per mL = unacceptable level of contamination. P value >0.05 is considered statistically not significant. |
||||||
Table 6 shows the gram characterization and frequency of bacterial contaminants on the lenses and handles of eye glasses of the study participants. On the handles, the most frequent organism was the Coagulase negative Staphylococcus Species (30%), while the least was the Proteus mirabilis (6%). On the other hand, coagulase positive Staphylococcus aureus (31%) was the most frequent organism found on the lenses, while Proteus mirabilis (10%) was the least frequent. There was no significant difference in the frequency of bacterial contaminants found on eyeglass handles compares to the lenses (P>0.05). However, the percentage of S. aureus found on the both the handles and lenses was significantly higher (P<0.05) than P. mirabilis which was the least isolated.
Table 6: Gram characterization and frequency of bacterial contaminants on lenses and handles of the eye glasses of the study participants.
Gram reaction |
Bacterial Isolates |
Hand les |
Lens |
Total |
P–value |
Positive |
Coagulase positive S. aureus |
23 (23.0)* |
31 (31.0)* |
54 (54.0) |
> 0.05 |
Coagulase negative S. species |
30 (30.0) |
22 (22.0) |
52 (52.0) |
> 0.05 |
|
Negative |
Bacillus species |
11 (11.0) |
14 (14.0) |
24 (24.0) |
> 0.05 |
Escherichia coli |
15 (15.0) |
11 (11.0) |
26 (26.0) |
> 0.05 |
|
Klebsiella pneumoniae |
16 (15.0) |
12 (12.0) |
28 (28.0) |
> 0.05 |
|
Proteus mirabilis |
6 (6.0) |
10 (10.0) |
16 (16.0) |
> 0.05 |
|
There was no significant difference in the frequency of bacterial contaminants found on eyeglass handles compares to the lenses (P>0.05). However, the percentage of S. aureus found on the both the handles and lenses was significantly higher (P<0.05) than P. mirabilis which was the least isolated. |
|||||
Table 7 shows the risk factors associated with bacterial contamination. All participants agreed to exposure of their glasses to dusty environment. Although all of them indicated that they have a glass case for keeping their glasses, only 43% of them keep their glasses in the case all the time, while 57% of them do so very often. 87% of the participants indicated that they cleaned their glass case all the time. 68% clean their eyeglasses often, while 32% do so more often. 18% of participants agreed to cleaning only the lenses, while 82% agreed to cleaning both the handles and lenses of their glasses. Furthermore, 91% of participants used running water as the solution in cleaning their glasses, while 9% use liquid lens cleaner. All participants (100%) agreed to use the lens cleaner material to clean their glasses. When asked about history of any signs and symptoms, 3% indicated red eye, 34% indicated itchy eye, 3% indicated painful eye, 16% indicated ocular discharge, 12% indicated eye strain, while 32% had no history of any signs and symptoms. All participants agreed to washing their hands always after using the toilet. With regard to frequency of eye check–up, 91% indicated that they go less often, while 9% of the participants go often. When asked to grade their compliance with eye glass care and maintenance, 34% indicated a very good level of compliance, while 66% indicated excellent level of compliance.
Table 7: Risk factors associated with bacterial contamination of eye glasses.
Characteristics |
Responses |
No. of Participants N (%) |
No. with contaminated eye glasses N (%) |
Do you expose your eye glasses to dusty environment? |
Yes |
100 (100) |
100 (100) |
No |
0 (0) |
||
How often do you keep your eye glasses in its case when not in use? |
Less often |
0 (0) |
100 (100) |
Often |
0 (0) |
||
Very often |
57 (57.0) |
||
All the time |
43 (43.0) |
||
How often do you clean the case for your eyeglasses? |
Less often |
0 (0) |
100 (100) |
Often |
0 (0) |
||
Very often |
13 (13.0) |
||
All the time |
87 (87.0) |
||
How often do you clean or wipe your eyeglasses |
Less often |
0 (0) |
100 (100) |
Often |
68 (68.0) |
||
More often |
32 (32.0) |
||
Which part of the eye glasses do you clean? |
Lenses only |
18 (18.0) |
100 (100) |
Handles only |
0 (0) |
||
Both |
82 (82.0) |
||
Which solution do you use for cleaning your eye glasses? |
Mouth breath |
0 (0) |
100 (100) |
Saliva |
0 (0) |
||
Running water |
91 (91.0) |
||
Liquid soap |
0 (0) |
||
Liquid lens cleaner |
9 (9) |
||
What material do you use for wiping your eye glasses? |
Handkerchief |
0 (0) |
100 (100) |
Tissue paper |
0 (0) |
||
Paper towel |
0 (0) |
||
Napkins |
0 (0) |
||
Part of my clothes |
0 (0) |
||
Lens cleaner material |
100 (100) |
||
Do you have history of any of the following signs/symptoms? |
Red eye |
3 (3.0) |
100 (100) |
Swollen eye |
0 (0) |
||
Itchy eye |
34 (34.0) |
||
Painful eye |
3 (3.0) |
||
Foreign body sensation |
0 (0) |
||
Ocular discharge |
16 (16.0) |
||
Eye strain |
12 (12.0) |
||
None |
32 (32.0) |
||
Hand hygiene after toileting |
Wash always |
100 (100) |
100 (100) |
Wash often |
0 (0) |
||
Wash less often |
0 (0) |
||
Never |
0 (0) |
||
How often do you go for eye check–up? |
Less often |
91 (91.0) |
100 (100) |
Often |
9 (9.0) |
||
Very often |
0 (0) |
||
Grade your compliance with eyeglass care and maintenance |
Very poor |
0 (0) |
100 (100) |
Poor |
0 (0) |
||
Good |
0 (0) |
||
Very good |
34 (34.0) |
||
Excellent |
66 (66.0) |
Figure 1 and 2 shows the antibiotic sensitivity pattern of Gram positive and Gram negative bacterial isolates recovered from the eyeglasses of the study participants. S. aureus was most sensitive (96.8%) to ciprofloxacin and gentamycin, but least sensitive (3.2%) to streptomycin, nalidixic acid, perfloxacin and cotrimazole. Coagulase negative Staphyloccocus species were most sensitive (95.5%) to chloramphenicol and erythromycin, but least sensitive (0%) to streptomycin and cotrimazole. Bacillus species were most sensitive (85.7%) to ciprofloxacin, chloramphenicol, tetracycline, gentamycin and amoxycillin, but least sensitive (7.1%) to streptomycin, nalidixic acid, perfloxacin and cotrimazole. Gram negative bacterial isolates on the other hand also show the same pattern, with most of them sensitive to ciprofloxacin, chloramphenicol and tetracycline (80–100%) and least sensitive to erythromycin (18.2–40%).
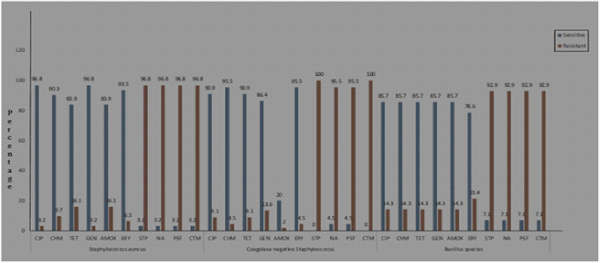
Figure 1: Histogram showing the antibiotic sensitivity pattern of Gram positive bacterial isolates recovered from the eye glasses of the study participants.
KEY: CIP= Ciprofloxacin, CHM= Chloramphenicol, TET= Tetracycline, GEN= Gentamycin, AMOX= Amoxycillin, ERY= Erythromycin, STP= Streptomycin, NA= Nalidixic acid, PEF= Pefloxacin, CTM= Cotrimazole.
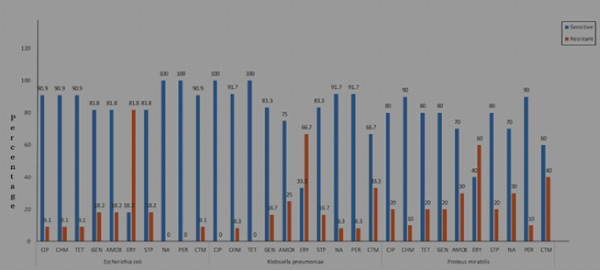
Figure 2: Histogram Showing Antibiotic Sensitivity Pattern of Gram Negative Bacterial Isolates Recovered from the Eye Glasses of the Study Participants.
KEY: CIP= Ciprofloxacin, CHM= Chloramphenicol, TET= Tetracycline, GEN= Gentamycin, AMOX= Amoxycillin, ERY= Erythromycin, STP= Streptomycin, NA= Nalidixic acid, PEF= Pefloxacin, CTM= Cotrimazole
Eyeglasses may act as possible carriers for bacteria that might infect the eyes. As stated by Wilcox [3], bacterial contamination of eyeglasses, particularly the lenses and handles, has been linked to ocular infection.This institutional based study was designed to determine the bacteriological quality of eye glasses of staffs and students of Babcock University, Ogun State. The study specifically seeks to determine the extent of bacterial contamination, the distribution of bacterial contaminants, identify associated risk factors, as well as determine the antibiotic sensitivity pattern of bacteria pathogens recovered from the eye glasses of the study participants.
The result of this study show that all the eyeglasses (100%) examined had bacterial contaminants, unlike the works of Butt et al. [4] and Osaro–Matthew et al. [11], who reported bacterial contaminants in 95.0% and 93.4% of the eyeglasses examined, respectively. The types of bacterial contaminants present on the eyeglasses examined in this study (Escherichia coli, Staphylococcus aureus, Proteus mirabilis, Bacillus species, Klebsiella pneumoniae and coagulase negative staphylococcus) differ somewhat from those of Butt et al. [4], who reported S. epidemidis and S. haemolyticus in addition to S. aureus.
Bacterial genera observed in this present work is however similar to those of Osaro–Matthew et al. [11], who reported Streptoccocus and Pseudomonas species in addition to E. coli, Bacillus species, Klebsiella species, S. aureus and coagulase negative staphyloccocus species observed in this study. With regard to the frequency of bacterial contaminants, Gram positive organisms with the highest and lowest occurrences in this study were Staphylococcus aureus (54%) and coagulase negative staphylococcus (52%), respectively who agrees with the work of Osaro–matthew et al. [11], who reported the same, 28.3% and 9.4%, respectively. On the other hand, Gram negative organisms with the highest and lowest occurrences were Klebsiella species (28.0%) and Proteus mirabilis (16%), respectively.This differs from the work of Osaro–matthew et al. [11], who reported Escherichia coli (51.9%) and Klebsiella species (1.89%).
In this study, staff eyeglass handles (54.2%) and lenses (25.0%) have more unacceptable level of bacterial contamination when compared those of the students, 47.4% and 17.1%, respectively. This is consistent with the work of Osaro–matthew et al. [11], who reported a higher occurrence on staff eyeglass handles (47.17%) and lenses (43.40%), against the 30.19% and 32.08%, respectively, observed on students’ eyeglass handles and lenses. This could be attributed to the fact that most staffs were parents, and may be too busy to take care of their eye glasses unlike the Students that are more privileged to only care for themselves and their studies. This is in line with the research done by Nwaugo et al. [8] who also shared similar views
Furthermore, male eyeglass handles (57.6%0 and lenses (21.2%) have more unacceptable level of bacterial contamination when compared those of the females, 44.8% and 17.9%, respectively. This is also in harmony with the report of Osaro–matthew et al. [11], who observed 52.83% and 50.94%, respectively among male eyeglass handles and lenses, respectively, as well as 26.42% and 22.64% among female eyeglass handles and lenses, respectively. According to Nwaugo et al. [8], who worked on fungal contamination of eye lenses, explained that male eye lenses are more contaminated than the females because they engage in more outdoor works/ activities than the females.
Comparison of bacterial contamination of eyeglass surfaces shows that the handles are more contaminated than the lenses. This also agrees with the observation of Osaro–matthew et al. [11]. This can be as a result of the fact that the hands are often employed to adjust the glass handles at intervals unlike the lenses, and pathogenic organisms harbored in the hands are easily transferred from the hands to the handle through touching. Also it was observed that most people clean only the lenses of their eye glasses and they leave the handles unclean forgetting the fact that it can harbor a large amount of microorganisms.
With regard to age, the highest unacceptable level of bacterial contamination was observed among participants who were between 46–55 years (27.3%). These are Staff members of the University, who may not have enough time for eyeglass care and maintenance due to their tight schedules. The observation in this study however disagrees with that of Nwaugo et al. [8], who observed a higher occurrence of fungal contamination among eyeglasses of Patients attending optometry clinic at Abia State University, Uturu, Nigeria, age 21–30 years (30.97%). Furthermore, from this study, it was also observed that the percentage of the recommended glass lenses (21.3%) and handles (81.6%) with unacceptable level of bacterial contamination were more than those of the Non–medicated eye glass lenses (12.0%) and handles (18.4%). This observation is a worrisome and therefore calls for more personal hygiene and eyeglass care by users of recommended eyeglasses.
With regard to risk factors associated with bacterial contamination of eyeglasses, majority of the participants (91%) clean their glasses with running water, while the remaining 9% use lens cleaner. The implication of this is that their eyeglasses are not properly disinfected as water in itself, does not possess antibacterial properties. Even though most people are of the opinion that using lens cleaner materials was the best option, the outcome of this study cast doubt on that belief. This finding concurs with that of Osaro–Matthew et al. [11], therefore washing of the lens cleaner materials properly and frequently is necessary to maintain the hygiene of eyeglasses. In this study, Coagulase positive Staphylococcus (a normal flora of the nasopharynx) had the highest frequency of occurrence, and this shows that the participants might have made use of handkerchief meant for cleaning the nasal area to clean their eyeglasses at one point or the other, thereby transmitting S. aureus to the glasses (handle/lens). In addition, since some people are known to intentionally or unintentionally blow their nostrils with bare hands without washing afterwards, Coagulase positive Staphylococcus can be easily spread from one person to another by hand shaking.
On the other hand, Coagulase negative staphylococcus species, especially S. epidermidis has long been thought to be non–pathogenic and is typically seen on the skin of many healthy individuals, their role as pathogens and their dramatically rising incidence rate have just recently come to light [18]. This can be a result of broader population hygiene issues. Most Nigerian populace do not always wash their hands well with soap and water after using the restroom, or even after eating or performing housework and due to the fact that human hands still contain a lot of pathogenic organisms even after thorough hand washing, when they are not adequately cleaned or sanitized, they serve as an ideal vehicle for the spread of bacteria to other locations and surfaces, particularly on eyeglasses for those who wear them.
Bacillus species were also present on the surfaces of the eyeglasses and these are spore formers, explaining why they are found everywhere. Due to the spore formation which enables them to survive in all environments, they have the ability to colonize surfaces [3].Proteus mirabilis are normally found in the gastrointestinal tract and has been implicated in contaminated surfaces due to poor toilet and hand hygiene. As an opportunistic microorganism, it is most times frequently resistant to antibiotics [19].
About 5% of healthy people typically have Klebsiella Pneumoniae in their respiratory tracts and feces.
In immunosuppressed patients, infection with this organism can result in bacteremia with a localized lesion. In addition, it is second only to E. coli in terms of urinary tract pathogens and it is among the top 10 bacterial pathogens that cause hospital–acquired illnesses [20, 21].
E. coli is a Gram–negative motile bacteria that naturally inhabits the digestive tract, but it has also been isolated from blood, pus, urine, cerebrospinal fluid, and other bodily fluids. It is known that specific E. coli strains can induce diarrheal illnesses. The organism is one of the main agents that can cause meningitis and bacteremia in newborns, as well as the most harmful organism implicated in urinary tract and wound infections in people [22].
For the antibiotic sensitivity pattern of the bacterial isolates recovered from the eyeglasses of the study participants. S. aureus was most sensitive (96.8%) to ciprofloxacin and gentamycin, Coagulase negative staphyloccocus species were most sensitive (95.5%) to chloramphenicol and erythromycin, bacillus species were most sensitive (85.7%) to ciprofloxacin, chloramphenicol, tetracycline, gentamycin and amoxycillin. Klebsiella Pneumoniae, E. coli, and Proteus mirabilis were most sensitive to ciprofloxacin, chloramphenicol and tetracyclin (80–100%). This pattern was different from the sensitivity pattern reported by Osaro–matthew et al. [11], in which E. coli was most sensitive to ceftriazone (96.4%), Staphylococcus aureus was most sensitive to gentamycin (100%), Coagulase negative staphylococcus Species was most sensitive to ofloxacin and peflacin (100%), while Klebsiella species was most sensitive to ofloxacine, peflacin, ceftriaxone, gentamycin, ceporex (100%). This shows that the antibiotic sensitivity pattern of bacterial pathogens is constantly evolving, hence the need for continuous antibiotic sensitivity pattern monitoring and surveillance to combat the menace of emergence and re–emergence of antibiotic resistance as recommended by past studies [23–25].
The outcome of this present study shows that more of the eyeglass lenses (25%) and handles (54.2%) of the Staff examined had unacceptable level of bacterial contamination (>105 CFU per mL) than those of the Students, 17.1% and 47.4%, respectively. Risk factors associated with bacterial contamination of eyeglasses as observed in this study include: exposure of glasses to dusty environment, irregular cleaning of eyeglasses, not using recommended liquid lens cleaner, poor compliance with eyeglass care and maintenance. And consequent upon these, the following measures are hereby recommended: Personal hygiene, especially hand cleaning after each visit to the toilet, regular cleaning of eyeglasses with recommended disinfectants of reputable quality, high compliance with standard eyeglass care and maintenance practice, and regular visit to the eye clinic for routine check–up.
The authors gratefully acknowledge the cooperation of staffs and students of Babcock University, who participated in the study.
All authors declare that ‘written’ informed consent was obtained from the participants with assurance of anonymity and confidentiality before the commencement of the study.
Ethical approval for the study was obtained from the Babcock University Health Research Ethics Committee (BUHREC), Babcock University, Ilishan–Remo, Ogun State, Nigeria, with the Institutional Review Board (IRB) number: BUHREC484/18.
Researcher has declared that no competing interests exist.