Pyrexial illness is a presentation associated with tropical environments, include many common infections, like influenza and tuberculosis that occur across the countries. Tropical fevers are defined as infections prevalent in or are unique to tropical & subtropical regions. Some of these occur throughout the year and some especially in rainy and post-rainy season. Febrile patients may also have chronic or recurrent medical problems unrelated to tropical exposure, non-infectious disease e.g., autoimmune, or malignant conditions.
Currently India is battling outbreaks of multiple viral and bacterial fevers like Covid 19, Dengue, Chikungunya, Swine Flu(H1N1), Enteric fevers, Monkeypox, tomato fever, Nipah and Zika virus fevers, Chicken pox, Measles, Scrub Typhus, Leptospirosis, West Nile fever, Brucellosis etc. across cities and states. While Public Health approach looks at Tropical Fevers as diseases classified based on Incubation Period, Types of exposure and transmission methods for Control & eradication goals.
Clinicians in smaller settings at sub-state capital towns and villages, with limited diagnostic facilities must depend upon Syndromic approach for management. With about 50 outbreaks and more than thousands of cases, currently common febrile conditions in India demand, more clinical acumen though supplementation by diagnostics in most urban areas.
This review is based on the clinician’s approach to manage Tropical fevers.
Materials and Methods: This review is based on the clinical syndromic approach and empirical treatment followed in smaller setting in India. It uses the burden of different fever cases, based on data available from multiple sources, challenges in real time data collection, lack of transparency and availability in public domain and outbreaks data of last 3 years from Integrated Disease surveillance Program for which author had worked in 2006-2013.
Key Words: Fevers; Tropical Fevers; Viral Fevers; Fever Panel of Diagnostics
An elevation of body temperature exceeding the normal daily variation is called Fever and it occurs in conjunction with an increase in hypothalamic set point. A body temperature of >106.7F is called Hyperpyrexia, that develops in patients with severe infections and bleeding (haemorrhages) in central nervous system (CNS). A variety of microorganisms called bacteria, viruses and Rickettsia cause systemic inflammation or infection producing fever. Other causes of fever are haemorrhage, trauma, tumours, or hypothalamic malfunction. Pyrexial illness is a presentation of many diseases particularly associated with tropical environments, and many common infections, like influenza & TB. Febrile patients may also have chronic or recurrent medical problems unrelated to tropical exposure, non-infectious disease e.g., autoimmune, or malignant conditions.
Common causes of fever include infections of the respiratory tract, GI tract, CNS and exanthems fever. Infection of the upper airways is the most common acute illness -Pneumonia, Asthma, bronchitis etc. encountered in the outpatient of smaller settings predominately during annual winter epidemics. The infection is more commonly caused by viruses including rhinoviruses, influenza viruses, parainfluenza, and respiratory syncytial viruses. Bacterial infection such as acute rhinopharyngitis, uncommon but presents with persistent symptoms of an URTI lasting over a week or worsening course after initial improvement or acute onset with high fever and inflammatory changes confined to the pharynx. Fever is common in both bacterial and viral gastroenteritis also. High fever is commonly present in Shigella, Salmonella, Shiga toxin-producing E. coli infections. Fever is low-grade in enteropathogenic and E. coli, cholera, TB meningitis and mid-ear infections (Otitis media) all types of Viral Hepatitis (A, B, C, E) and HIV/AIDS. Fever in Central Nervous System (CNS) infection (meningitis-bacterial, viral, encephalitis-viral) is the commonest presenting symptom in children beyond a month’s age owing to the presence of inflammatory mediators, particularly IL-1 and TNF in the blood or within the CNS. In MCD, fever was the first symptom in children younger than 5 years and 94% developed fever at some point. Fever with rashes (Viral exanthems) are common causes in children seeking care in smaller settings or OPD of bigger institutions, caused by more than 50 viral agents. Among them the first comes measles, then Chicken pox, scarlet fever, rubella in India etc [13]. Leptospirosis outbreaks caused by Leptospira a spirochaetal bacterium, through contaminated water or soil by infected animal urine, are very common during rainy season due to stagnation of water and people walking around barefoot in Mumbai, Mangalore etc.
Infections prevalent in or are unique to tropical & subtropical regions are called as Tropical Fevers (TFs). Some of them occur throughout the year & some especially in rainy & post-rainy season. Currently India is going through surplus rains and is battling outbreaks multiple viral and bacterial fevers like Covid 19, Dengue, Chikungunya, Swine Flu (H1N1), Enteric fevers, Monkeypox, tomato fever, Nipah and Zika virus fevers, Chicken pox, Measles, Scrub Typhus, Leptospirosis, West Nile fever, Brucellosis etc. across cities and states [1,2]. On an average around 40-50 outbreaks are reported to central surveillance unit (CSU) in national centre for disease control (NCDC) on weekly basis [2]. While there were only 2 outbreaks (1-Measles-1, & 1 ADD) in the first week of 2022, week 8 had 9 outbreaks with 7 of them showing symptoms of fever and week 15 had 12 outbreaks of which 8 reported fevers due to different conditions. Latest week of 21 week (latest week for which data is available in public domain) had 45 outbreaks and 32 of them were responsible for fevers.
In the past 55 years, since I graduated as medical professional in 1967, the researchers have identified about 1,500 new pathogens of them, about half are viruses, and over 75% of these are zoonoses (i.e., they have animal reservoirs from which they spread in humans).” Monsoons tend to be the peak season for influenza, and several viral respiratory tract infections appear to peak during this time of the year in India. Around 80 cases of Tomato fever have been reported in Kerala, Tamil Nadu, and Karnataka. It causes rashes or blisters, skin irritation and dehydration. Other symptoms include change in the colour of hands or legs, fatigue, coughing, nausea, vomiting, diarrhoea, stomach cramps, joint pain, headache, and body soreness. In July 2022 cases of Zika virus were silently spreading across Kerala, Uttar Pradesh, Maharashtra, Telangana, Jharkhand, Rajasthan, Punjab, and Delhi. Cases of hand, foot, and mouth disease (HFMD) were recently reported in pre-primary children specially children under 5 years of age and it can last for around 7-14 days in some Uttarakhand schools.
WHO identifies Chagas Disease, Cysticercosis, Dengue Fever, Dracunculiasis (GWD), Echinococcosis, Fascioliasis, Human African Trypanosomiasis (Sleeping Sickness) and Leishmaniasis as Tropical fever conditions [3]. Dengue, Scrub typhus, Encephalitis, Leptospirosis, and Malaria are the major tropical fevers in Indian ICUs. Infections in tropics often present as undifferentiated fevers with organ failures.
Despite an integrated Disease surveillance system (IDSP) since 2004-05, the real time data is captured for only the outbreaks by districts (726 of them) weekly. Most of this data too is from public sector and mostly from Rural India. The Urban outbreaks data flow from either Urban local bodies or respective district surveillance units is mostly from government institutions. As about 2/3 urban patients seek care from private sector information is limited. Thirty two of the 45 outbreaks reported in 21st week of 2022 had reported cases with fevers.
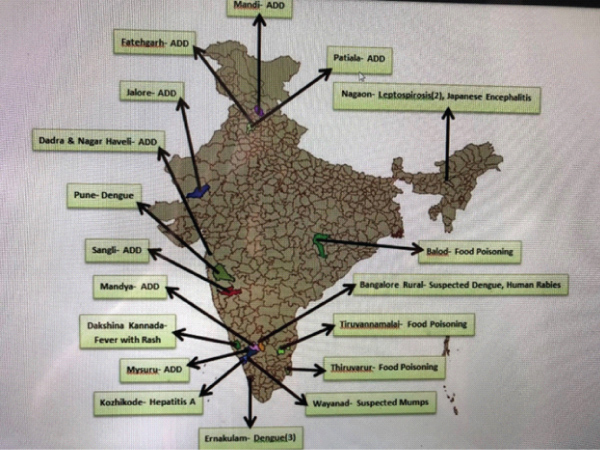
Figure 1: Map of Outbreaks reported in 25th Week (20-26 June 2022)- INDIA
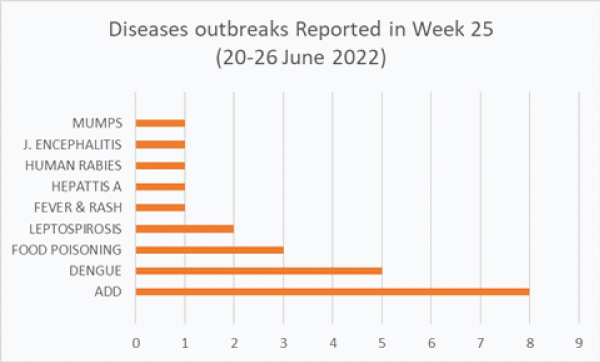
Figure 2: Outbreaks by Conditions in 25th Week 2022
The trends of the outbreaks in first half of last 3 years indicate that current year is witnessing more outbreaks of conditions causing fevers apart from Covid 19 pandemic.
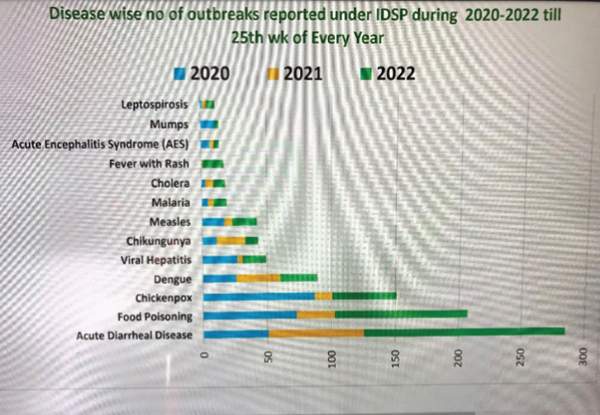
Figure 3: Trends of Outbreaks 2020-22
Table 1: Indian Burden of Fever cases in 2020-2022 by Conditions.
Disease |
2020 |
2021 |
2022 till July |
Malaria |
254,303 |
160,000 |
108821 |
Covid 19 |
10,286,329 |
24602803 |
9468414 |
Dengue |
44,585 |
44585 |
601102 |
Chikungunya |
43,424 |
43424 |
58515 |
Acute Encephalitis Syndrome |
5,487 |
707 |
427 |
Kala-Azar |
2,052 |
2052 |
884 |
Acute Respiratory Infection |
23,671,178 |
|
|
Enteric Fever (Confirmed/Suspected) |
106972/4775536 |
30934/1380955 |
|
Pneumonia |
422,250 |
|
|
Viral Hepatitis (All Cases) |
114,609 |
|
|
Tetanus |
4,884 |
|
|
Diphtheria |
1,991 |
|
|
Measles |
12,801 |
|
|
Viral Encephalitis (Including JE) |
23,189 |
|
|
Syphilis |
17,787 |
|
|
Meningococcal meningitis |
2,266 |
|
|
Whooping Cough |
11,985 |
|
|
Tuberculosis |
16, 28,161 |
1933381 |
223913 |
Total |
34,664,817 |
24,853,571 |
10462076 |
Source: Health Status Indicators- National Health Profile, CBHI, IDSP, NVBDCP MOH & FW Annual Report 2021-22, July 2022 |
|||
Reported conditions presenting fever as the only or one of the symptoms is around 35 million cases per year in India. We also must acknowledge this data is mostly from public sector facilities and that too primary and secondary care facilities. Tertiary care facilities and even secondary and primary private facilities hardly report to the surveillance system. With my experience of IDSP I can say at the most we may be capturing about 60% of the fever cases in the system. The IDSP over last 18 years has not been able to enforce reporting from the facilities listed already. This is one of the reasons for missing outbreaks in initial stages.
In Karnataka the home state (Province) of the author 2022 is seeing a greater number of Dengue fever cases. The state has reported over all 4405 cases till week ending 14 August 2022, of which 1154 (26%) are from Bengaluru city itself. The State added 1,354 cases to this year’s dengue tally in July alone. In 2021, the State had reported 7,189 cases and five deaths. Bengaluru’s dengue tally has reached to 950 as on 17 August 2022 from 351 cases in July 2022. Bengaluru had reported 9029 cases in 2019, 2047 in 2020 and 1643 in 2021 [6]. Ten Major hospitals in the city including State-run Victoria and K.C. General Hospitals see over 20 patients every day with viral fever and of these, on an average 10 test positive for dengue and four-five require admissions every day in the last 2 weeks. Among districts other than Bengaluru Mysuru with 445 cases, followed by Udupi (409), Dakshina Kannada (224), and Chitradurga (199) are reporting Dengue cases since beginning of June 2022 following heavy rains. As of 24 August 2022, the state has seen about 1200 confirmed Chikungunya cases out of over 32,000 suspected cases, half of them subjected to tests and 10% positive.
Fevers can be classified based on their incubation periods into short (<10 days), intermediary (10-21 days), Long (more than 4 weeks and variable incubation period diseases. They are also classified based on the specific exposure or associations (vector borne, waterborne, airborne, sexually transmitted, food borne etc).
Another classification is based on the organisms responsible [8]:

Figure 4: Trends of Outbreaks 2020-22
Most practitioner go by the recording of the body temperature to manage [8]:
Table 2: Fevers classified based on Body Temperature.
Body temperature |
°C |
°F |
Normal |
37–38 |
98.6–100.4 |
Mild/low grade fever |
38.1–39 |
100.5–102.2 |
Moderate grade fever |
39.1–40 |
102.2–104.0 |
High grade fever |
40.1–41.1 |
104.1–106.0 |
Indian Society of Critical Care Medicine (ISCCM) includes dengue haemorrhagic fever, rickettsia infections/scrub typhus, malaria, typhoid, Leptospira bacterial sepsis and common viral infections like influenza. However, the most practical way of looking at fevers is a ‘syndromic approach’ to diagnosis and treatment of critical tropical infections. Indian Society of Critical Care Medicine (ISCCM) has identified six major clinical syndromes [4,]:
The Indian Medical Association, recommends a much simpler logarithmic approach:
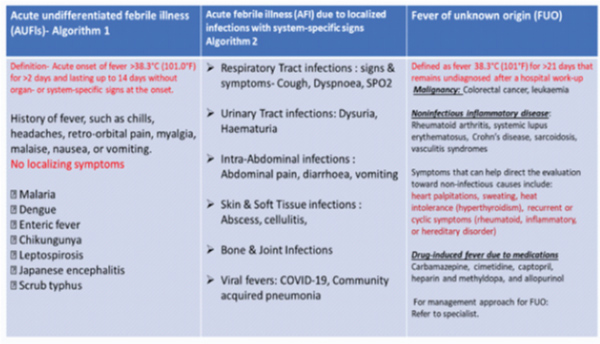
Figure 5: Fever-Logarithmic approach for Diagnosis & Management-IMA.
While more than 80% of fever cases are managed in outpatient care, some of them need hospitalization and few care in Intensive care units.
A prospective observational study done in 34 ICUs across India (July 2013–September 2014), among critically ill adults and children with non-localizing fever >48 h and onset < 14 days with any of the thrombocytopenia/rash, respiratory distress, renal failure, encephalopathy, jaundice, or multiorgan failure, could identify aetiology in 365 (80.5%) cases. Dengue (n = 105.23%) was the most common followed by scrub typhus (n = 83.18%), encephalitis/ meningitis (n = 44.9.6%), malaria (n = 37.8%), and bacterial sepsis (n = 32.7%) [4].
In another study of 454 hospitalized cases of Tropical fever over 3 years of 2014-2016, the key conditions with definitive diagnosis included Typhoid, Rickettsia fever, Dengue, Malaria and Leptospirosis. Trend indicated better case management resulting in a reduction in case fatality from 5.9% to 3.4% [5]
Evidence based algorithms; reliable rapid diagnostic modalities & early empiric therapy based on clinical syndromes used in India suggest possibilities of:
Undifferentiated fevers: Malaria (P. falciparum), scrub typhus, leptospirosis, typhoid, dengue, and other common viral illness.
Fever with rash/thrombocytopenia: Dengue, Rickettsia infections, malaria (Pf.), meningococcal infection, leptospirosis, measles, rubella & other viral exanthem.
Fever with Joint Pains: Chikungunya, Rheumatic Fevers, Influenza, Long Covid 19 (Flu-body’s immune response a protein to kill the virus.
Fever with ARDS: Covid 19, Scrub typhus, falciparum malaria, influenza including H1N1, leptospirosis, hantavirus infection, melioidosis, severe community acquired pneumonias due to Legionella spp. and Streptococcus pneumoniae and diffuse alveolar haemorrhage due to collagen vascular diseases.
Fever with multiorgan dysfunction: Bacterial sepsis, falciparum malaria, leptospirosis, scrub typhus, dengue, hepatitis A or E with fulminant hepatic failure and hepato-renal syndrome, Hanta virus infection, haemophagocytosis and macrophage activation syndrome
Febrile encephalopathy: Encephalitis (Herpes simplex virus encephalitis, Japanese B and other viral encephalitis), meningitis (S. pneumoniae, Neisseria meningitidis, Haemophilus influenzae, enteroviruses), scrub typhus, cerebral malaria and typhoid encephalopathy.
Algorithmic Approach Fevers with acute encephalitis syndrome:

Figure 6: Algorithmic Approach Fevers with acute encephalitis syndrome [12].
Currently the diagnosis and management of fevers heavily depends upon algorithmic approach especially in smaller settings. Involvement of meninges or encephalopathy is assessed, and case referred if need be.
The diagnosis is initially dependent on clinician’s experience and local epidemiology. Of late some towns and cities have both government and private laboratory facilities for establishing diagnosis, but the treatment is initiated without waiting for the results and modified if required based on the test results. The common tests done include 1) Blood smear microscopic examination for Malaria, Filaria Parasites, routine urine for pus cells or culture-for urinary infections, Non-structural protein 1 antigen detection (Rapid diagnostic Test Kits for Dengue, Malaria, Chikungunya etc) Serological Widal test or Blood culture for Typhoid. In the recent times 1) A Comprehensive Fever Panel by Multiplex PCR, costing about INR 6000 (US$-75) is a tropical fever panel is a group of blood tests that detects diseases such as Chikungunya, Dengue, Leptospirosis, Rickettsia, Malaria, Zika, and West Nile virus in the shortest turnaround time. 2) Fever Profile Maxi costing about half of that covers CBC, Urine Routine, ESR, MP profile, Typhi dot, Aerobic blood culture, CRP & Dengue Ns1. 3) Disease specific panels like i) Dengue Profile for INR 2000 including-Dengue-IgG, IgM, NS1 and Platelet count ii) Typhoid Profile for INR 2000 including- CBC, ESR, Urine Routine, Widal, Culture and Susceptibility from Blood and Typhi Dot iii) Leptospira Profile for INR Rs.2500 that gets Leptospira IgG & IgM Detection are becoming popular.
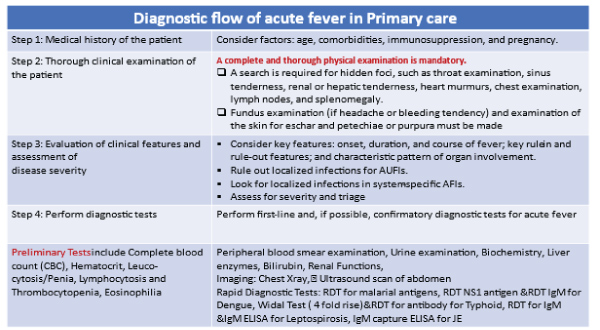
Figure 7:
Most primary (Family Physicians of all systems -Allopathy, Ayurveda, Homeopathy) care providers for follow syndrome-based empirical treatment:
Covid-19: Since April 2020, SARS-CoV-2 2 has become the predominant causes of fevers in India in past 2years and 8 months.
The initial tratment protocol and drugs recommended for every suspected cased based ARI symptoms was over-estimated even by the naitonal authorities as can be seen below:
Initila drug package list for each suspeced Covid 19 case:
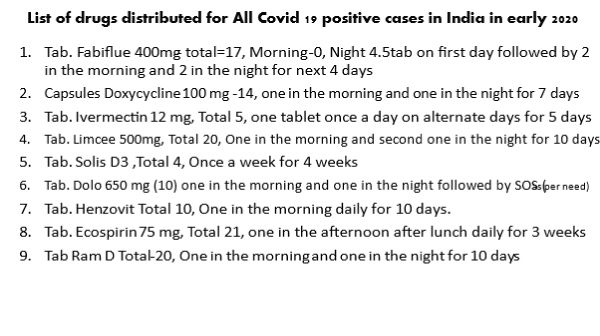
Figure 8:
My own effort of managing a Covid care centre (CC) in our apartment complex of 143 families, we had 36 cases (no deaths) between mid-2020 and till July 2022 and only 2 cases needed hospitalization and Oxygen support. Rest of the cases were managed by simple Paracetamol tablets and nasal decongestants. Two cases of long covid were encountered. While all had mild fever, sore throat, cough body ache, only 5 patients had loss of smell.

Figure 9:
Malaria
Causative organism: Plasmodium protozoa (P. falciparum, P. vivax, P. Malariae. [Odisha]). Plasmodium species are unevenly distributed across India. Orissa, Chhattisgarh, West Bengal, Jharkhand, and Karnataka contribute the most to the endemicity.
Vector: Anopheles mosquito.
Pathophysiology: Mechanical microcirculatory obstruction caused by cytoadherence to the vascular endothelium of parasitized RBC and sequestration, Intra-vascular haemolysis.
Clinical features: Paroxysm of fever, shaking chills and sweats occur every 48 or 72 h, depending on species. Hepatosplenomegaly may be present.
Manifestations of severe malaria: Cerebral malaria- Severe anaemia, Hypoglycaemia, Metabolic acidosis, Acute renal failure (serum creatinine > 3 mg/dl) & ARDS, Shock (“algid malaria”), DIC, Haemoglobinuria and 10. Hyperparasitemia (>5%).
Diagnosis: Microscopy: Thick smears for parasite detection; Thin smears for species identification.
Rapid diagnostic tests (RDTs) – Histidine rich protein, lactate dehydrogenase antigen based immune-chromatography (Level IA)- Sensitivity and specificity > 95%. Malaria ruled out if two negative RDTs.
Treatment: 1. Artesunate (Level IA)- Dose: 2.4 mg/kg i.v. bolus at admission, 12 h and 24 h; followed by once a day for 7 days + Doxycycline 100 mg 12 hourly. 2. Alternative: Quinine 20 mg/kg loading dose, followed by 10 mg/kg i.v. infusion 8 hourly + Doxycycline 100 mg 12 hrly. Clindamycin instead of doxycycline in pregnant women and children. (Level IA) Exchange transfusion is a treatment option for parasitaemia > 10%. (Not with Artesunate, Level IIA).
Dengue
Causative organism: Dengue virus (Flavivirus) serotypes.
Vector: Aedes Aegyptus mosquitoes. Dengue is endemic throughout India-resurgence of epidemics in past two decades.
Pathogenesis: Cross-reactive anti-dengue antibodies from previous infection enhance newly infecting strain with viral uptake of monocytes and macrophages. Amplified cascade of cytokines and complement activation, Endothelial dysfunction, platelet destruction and consumption of coagulation factors, Plasma leakage and haemorrhagic manifestations.
Clinical features: Incubation period 4-10 days.
Treatment: Isotonic fluid infusion just sufficient to maintain effective circulation during the period of plasma leakage; guided by serial haematocrit determinations (Level IA).
Blood transfusion is done only with overt bleeding/rapid fall in haematocrit.
Leptospirosis
Leptospirosis was found to be one of the important causes for acute febrile illness in the central and eastern parts of Uttar Pradesh, Gujarat, Kerala, Tamil Nadu, Maharashtra, Karnataka, and Andaman & Nicobar Islands. Outbreaks of leptospirosis have been increasing in India for the past three decades. The positivity rate for the disease is notable in the southern part of India at 25.6%, followed by 8.3%, 3.5%, 3.1%, and 3.3% in northern, western, eastern, and central India, respectively out of nearly million suspected cases. A National Programme for Prevention and Control of Leptospirosis (NPPCL) was launched in 2015 in the endemic states of India Mumbai city is notoriously popular for outbreaks after rains every year. It is a major neglected public health problem as underreporting is high. History of contact with rains, animals and contaminated water/environment is reported in more than 80% of cases and commonest symptoms include headache, fever, myalgia, and unexplained difficulty in breathing. It is an occupational hazard for people who work outdoors or with animals like Farmers, Mine workers. Sewer workers, Slaughterhouse workers, Veterinarians and animal caretakers, Fish workers, Dairy farmers, and Military personnel. As of end July 2022, about 4,000 suspected cases of leptospirosis were tested and of them, 95 were positive. In 2019, 6,851 were tested and 344 had tested positive. In 2020, 5,100 were tested and 319 had tested positive. In 2021, 6,005 were tested and 354 had contracted the disease in Udupi district of Karnataka.
Causative organism: Leptospira interrogans
Source of infection: Direct contact of skin or mucosa with water contaminated with urine or body fluid of an infected animal.
Peak incidence during the rainy season: Rampant in Mumbai, southern, western, and eastern India. Increasing incidence in “non-endemic” northern India
Pathophysiology: Leptospires multiply in the small blood vessel endothelium, resulting in damage and vasculitis and clinical manifestations.
Incubation Period: usually 5-14 days but can be 72 h to a month or more.
Clinical features:
Treatment: First line: Oral Doxycycline in uncomplicated infections. Penicillin G 1.5 MU 6 hourly for 7 days (Level IA), Alternative: Third generation cephalosporins. Plasma exchange, corticosteroids and intravenous (i.v.) Ig in selected patients (Level III) where conventional therapy does not work.
Enteric Fevers
Causative organism: Salmonella typhi, Serovar Para typhi A, B, or C
Transmission: focally contaminated food and water, most prevalent in urban areas, High incidence in children 15 years of age and younger starting from 2 -5 years
Pathophysiology: Bacteria spread throughout the reticulo-endothelial system and in areas of greatest macrophage concentration such as the Peyer's patches.
Incubation period: 1-14 days.
Clinical features/ Manifestations:
Treatment:
First line: Ceftriaxone i.v. 50-75 mg/kg/day for 10-14 days (Level IA) to cover MDR S. typhi. Azithromycin and Ciprofloxacin are alternatives. Consider dexamethasone 3 mg/kg followed by 1 mg/kg 6 hourly for 48 h in selected cases with encephalopathy, hypotension or DIC (Level IB).
The latest guidelines for 2022 recommend [11] -Ciprofloxacin, 500 mg twice daily orally or 400 mg twice daily intravenously for 5–7 days (10–14 days for severe typhoid). Azithromycin, 500 mg once daily orally for 7 days (for uncomplicated disease; not recommended for severe disease). Ceftriaxone, 2 g once daily intravenously for 10–14 days for severe typhoid.
Japanese Encephalitis
Causative organism: Japanese encephalitis virus,
Vector: Culex tritaeniorhynchus. Prevalent in Uttar Pradesh, Haryana, Bihar, Maharashtra, Andhra Pradesh, and Tamil Nadu.
Pathophysiology: Virus reaches the central nervous system through leukocytes and affects various parts of the brain to cause vascular congestion, microglial proliferation, formation of gliomesenchymal nodules, focal or confluent areas of cystic necrosis and cerebral oedema.
Clinical features: Incubation Period averages 6-8 days, with a range of 4-15 days. Prodromal period-fever, headache, vomiting and myalgia. Neurological features range from mild confusion to agitation to overt coma. Parkinson like extrapyramidal signs is common, including masklike facies, tremor, rigidity and choreoathetoid movements.
Diagnosis: IgM capture ELISA Serum: sensitivity 85-93%, Specificity 96-98%, CSF: Sensitivity 65-80%, Specificity 89-100%.
Treatment: Supportive-Airway management, seizure control and management of raised intracranial pressure.
Scrub Typhus
Causative organism: Orientia tsutsugamushi,
Vector: chiggers (larva of Trombiculid mite).
Prevalence: Outbreaks are reported from all over India starting from the sub-Himalayan belt to more eastern and southern Indian regions.
Pathophysiology: The organism infects vascular endothelium with subsequent vascular injury in organs like the skin, liver, kidneys, meninges, and brain resulting in multi organ manifestations.
Clinical Features: IP: 1-3 weeks: Fever, headache, and myalgia, breathing difficulty, delirium, vomiting, cough, jaundice
Complications: Pneumonia with ARDS – like presentation, hepatitis, aseptic meningitis, myocarditis and disseminated intravascular coagulation (DIC).
Lab Diagnosis (Serology): Weil-Felix: poor sensitivity and specificity, Indirect fluorescent antibody: “Gold standard” (Level IIA), Enzyme-linked immunosorbent assay (ELISA) for immunoglobulin G (IgG) and IgM antibodies: sensitivity and specificity > 90%.
Treatment: First line: Doxycycline 100 mg BD for 7 days (Level IA), Azithromycin or Rifampicin or chloramphenicol as alternatives in children and pregnant women. (Level IIB).
Swine Flu (H1N1)
The first confirmed case of swine flu H1N1 in India was documented in May 2009, and huge numbers of cases reported thereafter. In 2015, swine flu outbreak in India had led to significant morbidity and mortality. Incidences vary from State to State. As on 20th August 2022, 2401 are positive out of 12,604 persons tested for Influenza A H1N1 [Swine]. Substantial number of cases now being reported from Maharashtra (Mumbai and Pune), Karnataka (Bangalore) and Tamil Nadu (Chennai) are indigenous cases. Thirty-six laboratory confirmed cases have died.
Key Pandemics: Spanish Flu[A(H1N1)]1918-19; Asian Flu[A(H2N2)]1957- 59; Hong Kong Flu- [A (H3N2)] 1968-68; and “Swine Flu” [A (H1N1)] 2009-10. In the last 5 years the cases and deaths were 2017-38,811-2,270, 2018- 15,266- 1,128, 2019, 28,798 1,218, 2020- 2,752- 44, 2021-778- 12, and 2022 (till end July 22)-252, 12. The Maharashtra state-wide tally of H1N1 so far in 2022 is 142, including 23 in Pune and 22 in Palghar.
Causative organism: Influenzas virus belongs to Orthomyxoviridae Sub Types based on hemagglutinin (H) and the neuraminidase(N)- Presently circulating strains- [A (H1N1)2009; Circulating seasonal influenza A(H3N2) and Influenza B]. Cause Epidemics, seasonal Influenza outbreaks and sporadic cases. Incubation period -1-2 days, effect All ages: incidence higher in extremes of ages /both sex. India usually witnesses two peaks- 1. Jan- Mar & 2. Post monsoon (Aug – Oct). Management is symptomatic and supportive treatment.
Viral Fevers
Viral fevers are out numbering bacterial infections in the last few years in India. Causative Organisms: Zika, Nipah, Ebola, Monkey Pox and Crimean-Congo haemorrhagic fever (CCHF).
Ebola virus disease (EVD): is a viral haemorrhagic fever of humans and other primates caused by Ebola viruses. Incubation period is 2-21 days. Signs and symptoms include a fever, sore throat, muscular pain, and headaches. Then, vomiting, diarrhoea and rash usually follow, along with decreased function of the liver and kidneys. Some people begin to bleed both internally and externally. The disease has a high CFR of 25-90% with an average of 50%.
CCHF: has sudden onset of fever, muscle ache, dizziness, neck pain, backache, headache, sore eyes, and photophobia (sensitivity to light). There may be nausea, vomiting, diarrhoea, abdominal pain, and sore throat early on, followed by sharp mood swings and confusion.
Zika fever: manifests as fever, rash, conjunctivitis, headache, malaise, and joint pains. Nipah virus fever is prevalent in West Bengal (Siliguri district). Transmitted to humans through contact with infected Pigs and Bats and eating fruits eaten by bats and birds.
Monkey Pox: Is a viral disease like smallpox. Symptoms include fever, headache, malaise, muscles and Backache and rashes on palms and hands. A total of 9 monkeypox cases and one death related to it has been reported in India so far.
All viral diseases have no specific treatment and are to be given symptomatic treatment.