Background: Healthcare personnel working in hospitals and healthcare institutions across the world are more vulnerable to occupational dangers than those working in other fields.
Aim: The review aimed to evaluate the current research literature on this topic and highlight different potential hazards healthcare professionals are exposed to. Furthermore, we provided recommendations on how to remove or mitigate such risks.
Methodology: Literature search was performed to make an over view, assess the incidence, and highlight on the different risk factors that healthcare professionals may encounter.
Discussion: Several studies and reviews indicated that the considerable number of healthcare workers worldwide are susceptible to occupational hazards in their work environment including injuries, biological risks, non–biological hazard, ergonomic risks, chemical risks, and psychological risks. Some of these occupational hazards are resulting from poor awareness and education, stress related conditions, and lack of proper personal protective equipment.
Conclusion: It was concluded that a considerable number of healthcare professionals are exposed to occupational hazards in different healthcare settings across the globe. Proper awareness and on job training may mitigate these hazards. The focus on risk assessment, quality management, and infection control will positively contribute in minimizing potential hazard exposure.
Keywords: Health Sector; Occupational Hazards; Incidence; Risk Factors; Recommendations.
A health care facility is a workplace that provides patients with diagnostic, treatment, and preventative services [1]. Health care employees are those who work in any health care facility [2]. According to the World Health Organization (WHO), health care institutions employ about 59 million people globally [3].
The WHO categorized health care employees into a variety of categories, including general and speciality medical practitioners, dentists, nursing and midwifery experts, pharmacists, and other allied health professionals. Health care workers at various health care institutions are at risk of a wide range of occupational dangers, including infections caused by sharps injuries, adverse exposure to radiation and toxic pharmaceuticals, injuries, physical aggression, and psychological stress. Though biological risks such as disease–causing agents (like viruses, bacteria, fungi and parasites) are well known across the world, non–biological hazards and their significance are frequently overlooked [4].
Occupational hazards endanger the health and safety of workers, and have a negative impact on the economy, accounting for around 4% of worldwide yearly gross domestic product (GDP) i.e., about 2.8 trillion dollars [5]. There is a widespread misunderstanding that healthcare facilities are “clean” and free of risks, despite the fact that chemical and blood–borne disease exposure can be career– and life–ending. According to statistics, a hospital is one of the most dangerous places to work; in the United States, hospitals had 253,700 job–related injuries and illnesses, which was greater than in construction and manufacturing industries. [6]
According to Amnesty International, more than 7000 health care workers have died as a result of COVID–19 [7]. Health care workers’ working environments are strongly connected to the quality of care provided to patients. Workplace circumstances, such as shift assignments, psychosocial variables, team management, working hours, and culture, are linked to health and safety results. [8] The protection of health care workers has the added benefit of promoting public health because they make up 10 to 18% of each country’s workforce [3]. This review aimed to address the occupational hazards in healthcare facilities, their incidence, risk factors, epidemiology, and how they affect healthcare professionals.
We searched literature data to investigate different occupational hazards in health care sector. Furthermore, the underlying effect, and incidence on healthcare workers were highlighted. The key words used in searching literature includes “occupational hazards”, “occupational risks”, “healthcare workers”, “healthcare professionals”, “occupational accidents”, “occupational health”, and “occupational injuries”. Information was collected from original and indexed review articles written in English language. Data was collected from electronic databases like Medline (https://www.nlm.nih.gov/), PubMed (https://pubmed.ncbi.nlm.nih.gov/), and Scopus (https://www.scopus.com/home.uri?zone=header& origin=) including the period from 2000 till the end of 2021. Furthermore, data were included from governmental and non–governmental organizations to identify different occupational hazards on healthcare working personnel.
The review addressed the following questions “what are the occupational hazards in healthcare settings, what are their risks, and do healthcare professionals aware about these risks?”. The inclusion criteria for the collected data were aimed to answer the mentioned questions and it was based on the following: Study topic is related to occupational hazard exposure, study participants are healthcare workers, experimental or an observational study, article published in a peer reviewed journal in English language. The collected studies were screened to ensure their eligibility for discussing the current review topic. The data was classified based on the type of hazard exposure per occupational level in the healthcare system.
The organizational and workplace characteristics of healthcare workers working at health facilities of Gondar city, Ethiopia with type of violence is presented in Table 1. The frequency of occupational health hazards of healthcare workers is presented in Table 2, while the occupational hazards types and its relation to different healthcare professionals is presented in Table 3.
Table 1: Organizational and workplace characteristics of healthcare workers working at health facilities of Gondar city, Ethiopia with type of violence, (n = 531) [9].
Variable |
Physical violence (%) |
Verbal abuse (%) |
Sexual harassment (%) |
Job position |
|||
Staff/service provider |
22.1 |
47.7 |
7.6 |
Ward/clinic head |
22.5 |
60 |
2.5 |
Coordinator |
14.3 |
71.4 |
0 |
Shift work |
|||
Yes |
28.6** |
62.2** |
8.6 |
No |
10.8 |
37.4 |
4.6 |
Experiences (in years) |
|||
1–5 |
54.3* |
65.2* |
97.4 |
6–10 |
31.4 |
23.8 |
0 |
11–15 |
3.4 |
2.1 |
0 |
16–38 |
10.9 |
8.9 |
2.6 |
Department |
|||
Inpatient departments |
54.7** |
42.2** |
52.6* |
Pharmacy/laboratory |
5.1 |
18.8 |
7.9 |
Emergency departments |
18.8 |
12.1 |
15.8 |
Other departments |
2.6 |
2.5 |
5.3 |
OPD |
18.8 |
24.5 |
18.4 |
Ownership |
|||
Private |
13.7* |
15.6 ** |
7.9 * |
Government |
86.3 |
84.4 |
92.1 |
Violence Reporting procedure |
|||
Available |
31.6 |
15.6 |
26.3 |
Unavailable |
68.4 |
84.4 |
73.7 |
Table 2: Frequency of occupational health hazards of healthcare workers [10].
Health Experiences of healthcare workers |
Frequency (n=200) yes (%) |
Biological hazards |
79 (39.5) |
*Sharp–related injuries |
43 (21.5) |
*Cuts and wounds |
34 (17) |
*Direct contact with contaminated specimens |
21 (10.5) |
*Airborne diseases |
18 (9) |
*Infectious disease and or Infections |
15 (7.5) |
*Other (blood borne pathogens, vector borne diseases) |
15 (7.5) |
Non–biological hazards |
63 (31.5) |
*Stress |
|
*Physical, psychological, social and or sexual abuse |
21 (10.5) |
*Musculoskeletal Injuries |
21 (10.5) |
*Slips, trips and or falls |
12 (6) |
*Fractures |
10 (5) |
*Others (chemical spills, noise, burns and radiation) |
20 (10) |
Table 3: Occupational hazards types and its relation to different healthcare professionals.
Hazard type |
Healthcare professional category |
Sharp–related injuries |
Nurses / Surgeons |
Cuts and wounds |
Nurses / Surgeons |
Direct contact with contaminated specimens |
Nurses / Surgeons |
Airborne diseases |
Nurses / Surgeons / Pharmacist / Physicians / Cleaning workers |
Infectious disease and or Infections |
Nurses / Surgeons / Pharmacist / Physicians / Cleaning workers |
Stress |
Nurses / Surgeons / Pharmacist / Physicians / Cleaning workers |
Physical, psychological, social and or sexual abuse |
Nurses / Surgeons / Pharmacist / Physicians / Cleaning workers |
Musculoskeletal Injuries |
Nurses / Cleaning workers |
Radiation |
Radiologist / Nurses |
Chemical / Chemotherapy |
Pharmacist / Nurses / Cleaning workers |
It is evident from Table 1 that 54.7% of physical violence, 42.2% of verbal violence, and 52.6% of sexual harassment occurs in the inpatient department. On the other hand, 54.3% of physical violence, 65.2% of verbal violence, and 97.4% of sexual harassment occurs for healthcare workers who’s experience within 1 to 5 years. Most of healthcare facilities lack proper procedures for reporting violence. Furthermore, the data indicate that occupational hazards incidence rate is low in private healthcare sectors compared to governmental healthcare facilities.
The frequency occupational hazard incidence showed to be 39.5% for biological hazards, from which 21.5% for sharp–related injuries followed by 17% for cut and wounds. Non–biological hazards incidence rate showed to be 31.5%, from which 21.5% for work related stress, 10.5% for physical, psychological, social and or sexual abuse, and 10.5% for musculoskeletal injuries (Table 2).
Different occupational hazards are related to different occupations in healthcare settings. Pharmacists are mainly susceptible to chemotherapy exposure and different chemical reagents during pharmaceutical compounding and drug administration. Furthermore, they are exposed to airborne diseases due to direct contact with patients in healthcare settings and community pharmacies. Working for a long time is exposing the pharmacist to stress and burnout problems.
Nurses are mostly susceptible to various types of hazards including sharp–related injuries, cuts, and wounds, direct contact with contaminated specimens, airborne diseases, stress, musculoskeletal injuries, physical, psychological, social, and sexual abuse. Surgeons are mainly exposed to sharp–related injuries, cuts, and wounds, and direct contact with contaminated specimens. Radiologists are exposed to radiations hazard effects (Table 3).
General Occupational Hazards
A multicenter study carried out on 438 health care workers in Saudi Arabia from which 60% of males and 40% of females showed that needle stick injuries (34.5%) and infections related to airborne illnesses (31.1%) were the most prevalent biological risks encountered by the health care workers. Work–related stress was the most prevalent non–biological hazard encountered (69.6%), followed by physical, psychological, sexual, and/or verbal abuse (52.7%), and musculoskeletal disorders such as muscular aches/strains/sprains (39.7%). In addition, the results showed that 300 health care workers (68.5%) were exposed to one or more biological hazards, while 384 health care workers (87.7%) faced one or more non–biological hazards [4].
A cross–sectional study was performed in Kampala city, Uganda. The study included 200 healthcare professionals from eight main health institutions. The results revealed that 50.0% of healthcare workers reported an occupational health danger. Among them, 39.5% were exposed to biological dangers, while 31.5% were exposed to non–biological hazards. The risk factors for encountering such hazards include; not wearing the essential personal protective equipment, working overtime, job–related demands, and working in numerous health institutions [11].
In 2016, regulatory authorities in Thailand explored 253 hospitals for job hazards. The regulatory report included survey results from 88667 health care workers in these hospitals. The results showed that 32 percent of health care workers indicated ergonomic risk issues in the workplace; 26 percent reported biological risk, 12 percent reported chemical risk factors, 18 percent reported psychosocial risk factors, and 18 percent reported dangerous working conditions. In terms of physical dangers, 5.9 percent recognized excessive heat as a risk factor in the work, 7.1 percent mentioned noise, and 12.4% indicated insufficient light [12].
In 2020, a cross–sectional study aimed to evaluate occupational hazards in Thailand hospitals. The study results showed that formaldehyde (55.1%), ethylene oxide (35.3%), cleaning chemicals (43.1%), glutaraldehyde (48.0%), anesthetic gas (80.0%), mercury (19.6%), lead (19.6%), hand cleansers (100.0%), and gloves or dust from powdered medical gloves (100.0%) were the chemicals to which healthcare workers were most exposed. Furthermore, 49.1% of healthcare professionals in the inpatient department were the most exposed to chemotherapy [6].
On the other hand, 86% of nutrition service healthcare professionals were most exposed to loud noise, 82.4% to heat, and 43.1% to cold, whereas 65.4% of surgery and anesthesia healthcare workers were most exposed to glare, 69.2% to poor lighting, 80.4% to radiation, and 42.3% to vibration. Besides, 60.1% of inpatient healthcare professionals were exposed to radiation and 21.9% for outpatient healthcare employees [6].
Comprehensive research looked at blood and blood–borne pathogen exposure rates among healthcare professionals in Sub–Saharan Africa. The lifetime prevalence of needlestick injury ranged between 22 and 95 percent, while the one–year prevalence was between 39 and 91 percent. According to two studies, 21 to 32% of healthcare workers showed inadequate knowledge or training in the prevention of needlestick injuries. Furthermore, in four trials, the rate of needle recapping ranged from 12 to 57% [13].
Cleaning has been linked to several ergonomic and chemical dangers that increase the risk of occupational harm. Research in the Canadian province of British Columbia looked into the epidemiology of occupational injury among cleaners in hospital work environments. The results showed that there were 145 injuries among cleaners, with an annual incidence rate of 32.1 per 100 person–years [13].
Female cleaners had a greater risk of sustaining all injuries and bruising than male cleaners. Part–time or casual employees had a decreased incidence of all injury, allergy, and irritation events. Cleaners with more than ten years of experience had a much–decreased chance of injury, bruise, allergy, and irritant events [14].
Cross–sectional research was undertaken with 370 healthcare personnel from three hospitals in Bhutan's western area. The data revealed that the prevalence of exposure to one or more asthmagens was 98.7%, carcinogens 28.1%, and ototoxic agents 7.6%. Besides, anesthetic gases accounted for 6.2% and antineoplastic medications accounted for 2.2% [15].
In the asthmagens individuals, the most prevalent exposures were to latex and cleaning and disinfecting chemicals; in the carcinogen’s individuals, formaldehyde; and in the ototoxic agents, p–xylene. Exposures were caused by the use of latex gloves, the use of bleach and chlorhexidine for cleaning, the use of formaldehyde as a disinfectant in the laboratory, and the use of p–xylene in the laboratory [15].
Occupational stress can cause immune function suppression or dysregulation. Fatigue, acute stress from sleep deprivation during night shifts, chronic stress from persistent disruptions in work/sleep schedules, lack of personal protective equipment, patient exposure, negative psychological stress, critical situation decisions, social stigma, and abuse due to public fears of infection are all factors that contribute to increased stress [16].
Although health care workers are susceptible to a higher probability of COVID–19 infection compared to the general population, it was shown that they were associated with lower mortality. This might be attributed to improved screening among health care workers and early care of non–severe disease cases [16].
In terms of medical worker protection in the twenty–first century and covid–19 era, medical gloves act as a barrier between healthcare professionals and potential hazards such as biological specimens from patients. To give additional protection, face shields can be used in conjunction with other protective measures such as face masks. Mouthwashes and throat gargling may be effective in lowering the viral load, but additional research is needed. Several covid–19 vaccines have now received extraordinary permission for usage, with effectiveness ranging from 50 to 95% [17].
A research study was performed in public health facilities in southern India. The study included 482 healthcare workers. The data revealed that thirty–nine percent of the workers did not detect work–related health dangers, but upon further investigation, they identified exposure to at least one hazard. Among the 81.5 percent who reported biological hazard exposure, 93.9 percent had direct skin contact with infectious materials. Seventy–five percent reported needle stick injuries experienced at least one in the preceding three months. Furthermore, lifting large things (42%) and standing for lengthy periods (37%), negative sentiments (20.3%), and verbal or physical abuse at work (20.5%) were among the ergonomic hazards. More than a third of healthcare workers were unable to identify work–related health dangers. The findings point to the necessity for behavioral change training [18].
A study showed that non–rotatory dizziness and neurovegetative symptoms were observed in pharmacists and nurses exposed to chemotherapy medications, with worry and stress being the most common extra–hearing complaints [19]. Thus, an emphasis should be done on wearing personal protective equipment (PPE) during pharmaceutical compounding and dose dispensing of antineoplastic agents. The PPE includes aprons, face masks, gloves, and face shields (Figure 1).
Employees in radiology and other healthcare departments may be exposed to chemicals used as cleaning agents and germicides, such as detergents, quaternary ammonium compounds, iodophor or phenolic–based germicides, and alcohol. The biggest risk linked with these products is contact dermatitis. Detergents and other surface cleansers or germicides can be irritants, and alcohol can defat the skin. Phenolic–based germicides may potentially have systemic effects due to adsorption via healthy skin [21].
The risk of high COVID–19 exposure is usually higher for healthcare workers due to increased admission to hospital, long–term exposure, failure to implement effective personal protection a lack of personal protective equipment (PPE), and a lack of training, supervision, and monitoring of infection prevention and control mechanisms [22].
Occupational Risk of acquiring Human Immunodeficiency Virus(HIV)
A study included healthcare workers who reported accidental exposures to infective material from acquired immunodeficiency syndrome (AIDS) patients in Brazilian healthcare facilities. There were 338 accidents reported by 247 health care personnel of which 50% were percutaneous and 22% were mucous membrane exposures to blood. An additional 404 health care personnel stated that they had no occupational exposure but want to be examined. The study examined 115 health care personnel with more than 6 months of follow–up from the 247 with at least one injury. None of the examined personnel tested positive for HIV antibodies [23].
Furthermore, the study showed that six (1.5%) personnel of the 404 health care personnel with no accident tested positive for HIV. The highest frequencies of accidental exposures were reported by nurses followed by physicians [23].
Workplace Violence
A study was conducted on 310 physicians from Ordu province, Turkey to investigate workplace violence. The study results showed that 93.2% of the physicians had experienced verbal abuse, 86.1% psychological violence, and 22.6% physical violence. Patients and their families were the most prominent source of violence. Those who have experienced violence exhibited much greater levels of emotional stress and depersonalization [24].
Burnout
Burnout is frequent in health care workers, particularly anesthesiologists in high–income societies. Burnout is caused by long–term job stress. Regarding low– and middle–income countries a study was conducted to address burnout rates among 160 anesthesia providers (physicians and non–physicians) working in private and public hospitals in Zambian. The study data showed that burnout was seen in 51.3% of participants. Burnout was substantially connected with not being a physician and not having a suitable team to work with [25].
Workplace Violence
A study that included 215 nurses from two hospitals in Turkey was conducted to explore workplace violence. The results showed that 73% of nurses said they have been sexually harassed. Physicians and patients were the primary culprits, and these situations were more prevalent in the in–patient clinics. Furthermore, 45% of nurses reported a decrease in job productivity as a result of these incidents [26].
A Study was conducted in a general hospital in southern Thailand that includes 545 nurses. The results of collected data over 12 months indicated that the incidence of verbal abuse was 38.9%, physical abuse 3.1%, and sexual harassment 0.7%. Patients and their families were the individuals who made verbal and physical abuse, while coworkers were the individuals who made sexual harassment. Working in high–risk settings like out–patient units, emergency rooms, operating rooms, medical and surgical units, and being younger were linked to an increased risk of violence [27].
Study results from 6 university hospitals including 441 nurses in Turkey revealed that 60.8% of nurses reported some type of workplace violence, with 59.4% reporting verbal abuse and 16.6% reporting physical assault. Data showed that 47.4% of verbal aggression was attributed to patients, 39.5% to visitors, and 10.7% to health staff. On the other hand, 14.3% of physical violence was attributed to patients, 5% to visitors, and 0.5% to health staff. Besides, 42.9% of nurses said it had a bad impact on their bodily and/or psychological health, and a negative influence on their work performance [28].
A study in China that included 886 nurses from 8 tertiary hospitals showed that 67.2% of nurses reported workplace violence. Workplace violence was linked to higher levels of anxiety and despair [29].
Blood–Borne Pathogens
From 3 tertiary care hospitals in Hunan Province in China, 441 nurses were included in a study showing that 82% of nurses reported a needlestick injury. These injuries were most commonly sustained when separating a needle and syringe, recapping a needle, transferring needles for disposal, and administering injections. Only 8% of the injuries were reported to authorities. When taking blood, delivering an injection, or beginning an intravenous line, the vast majority of nurses never donned gloves. 29% had not received Hepatitis B vaccination [30].
The study comprised 132 health care professionals from a chest hospital in Zagazig, Egypt, to explore the prevalence and risk factors of latent tuberculosis (LTBI). The results indicated that being a nurse, working for more than ten years, smoking, and diabetes were all linked to an increased risk of LTBI. The prevalence of LTBI was 28.8% and 59.1% using QFT–GIT and TST assays respectively [31].
Work Environment and Job Satisfaction
Baseline research included 3088 nurses from 12 hospitals in China, while a one–year follow–up study included 1521 nurses to investigate the work environment and job satisfaction level. Results showed that at the baseline study, the prevalence of intention to leave was 16.26%, and at one–year follow–up, the incidence rate was 14.46%. Intention to quit was connected with increased emotional pressure, lower workplace commitment, decreased meaning of work, and decreased job satisfaction [32].
According to Turkish research, 90% of nurses had at least one musculoskeletal complaint in the previous six months. The most prevalent type of discomfort was low back (69%), followed by the neck (54%), and shoulder (46%) [33].
Chemical Hazards
In nine hospitals in Istanbul, Turkey 171 nurses worked in cancer units and delivered antineoplastic medicines. Data showed that 94.7% of nurses reported using gloves all the time, 89.5% masks, 52.0% gowns, and 18.7% goggles. Besides, 40.4% reported preparing pharmaceuticals in a biological safety cabinet, 37.4% reported preparing drugs in the nurses' office, and 15.8% reported preparing drugs in a room that was also used for other purposes such as meals [34].
Chemical Hazards
A research study comprised 40 hospital pharmacists from Turkey who handled chemotherapy. The majority (42.5%) reported utilizing automated chemotherapy equipment, with 30% manually preparing the medications. Use of double gloves (63.6%), glasses (62.2%), hair cap (66.7%), foot coverings (32.3%), masks (89.1%), coat (92.1%), closed–system medication transfer set (70.6%), and biological safety cabinet (91.7%) was not always consistent with published standards [35].
Work Environment and Job Satisfaction
Pharmacists play an important role in assuring the appropriateness of pharmaceuticals given or delivered to patients, but they may be unable to do so if working circumstances are not optimum. Community pharmacists who work in chain pharmacies report significant levels of stress as a result of the volume of work they are required to do and the staffing levels [36].
A data analysis performed indicated that burnout is prevalent in 74.9% of community pharmacists. Burnout was reported by 68.9% of pharmacists due to emotional exhaustion, followed by 50.4% depersonalization and 30.7% decreased personal accomplishment. Shorter years of experience, working exclusively in a chain pharmacy, and a lack of support for burnout or resiliency were all major risk factors for burnout [37].
Driving and Use of Mobile Phones
It is well known that pharmacists working in the sales field are encountering several problems regarding the high use of mobile phones and driving for long hours and distances to different areas/locations for doing the marketing and sales job. A significant number of accidents occur as a result of falling asleep while driving under repetitive driving conditions. The scientific research on the danger potential of mobile phones when used in cars reveals a significant degradation of driving performance [38].
The review results indicated that there is a large portion of healthcare workers around the world are exposed to different hazardous conditions in their work facilities, especially during the pandemic of COVID–19. Exposure to these hazards may be correlated with different disease conditions that defiantly affect the healthcare professionals’ quality of life.
Some health care professionals are exposed to chemicals during their work. Some of these chemicals possess a potential risk of a carcinogenic effect. Thus, healthcare professionals should perform a periodical check on regular bases to detect any incidence of cancer. On the other hand, healthcare facilities need to alleviate and redistribute the workload on healthcare workers to avoid the risk of ergonomic hazards to the musculoskeletal system.
Poor quality management, absence of risk assessment, and lack of infection control measures are considered the main reasons for increasing occupational hazards in healthcare facilities. Thus, the focus should be on these areas to provide healthcare workers better work environment.
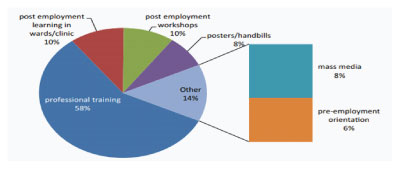
Professional and on–job training is essential for the mitigation of occupational hazards. A significant number of healthcare workers attributed their knowledge about occupational hazards to professional training. Additionally, radiologists and nurses are most commonly exposed to radiological hazards from x–rays, ultrasounds, mammograms, CT scans, and others. They should be trained well on special precautions to perform to avoid undesired effects of radiation on their health and wellbeing.
It has been found that a significant proportion of healthcare personnel is exposed to occupational dangers in various healthcare settings across the world. Proper knowledge and on–job training may help to reduce these risks. The emphasis on risk assessment, quality management, and infection control will all help to reduce possible hazard exposure.
None.
Author declares that there is no Conflict of interest.