Background: COVID–19 booster effectiveness against reinfections is not clearly known.
Objectives: To compare the clinical–epidemiological characteristics of the cases of reinfection by COVID–19 with booster versus with 1 or 2 doses, and to evaluate the relative effectiveness of the COVID–19 booster against reinfections in relation to only 1 or 2 doses of vaccine.
Methodology: An observational, longitudinal and prospective study of COVID–19 reinfections was conducted from March 1, 2020 to September 1, 2022, in a general medicine office in Toledo, Spain.
Results: 47 cases of COVID–19 reinfection were included, of which 15 were cases of COVID–19 reinfection with booster and 23 cases of COVID–19 reinfection with vaccine (1or 2 doses) but in these with 25 infections (2 cases presented 2 reinfections: 2 women aged 17 and 19, with 2 and 1 dose of the vaccine, respectively). The only statistically significant differences between COVID–19 reinfection with booster versus with only 1 or 2 doses of vaccine, were fewer women, more health care workers, fewer cases with chronic diseases, and more chronic diseases of the genitourinary group. There were no statistically significant differences in social, family, ethnic factors or year of reinfection. The vast majority of reinfections were symptomatic, all mild, and without statistically significant differences, although ENT symptoms clearly predominated in cases of COVID–19 reinfection with booster. COVID–19 booster effectiveness against reinfections versus only 1 or 2 doses, calculated as a percentage based on the formula: 1 – [COVID–19 cases incidence with vaccine booster / COVID–19 cases incidence without vaccine booster (only 1 or 2 doses of vaccine)] × 100, was 40%.
Conclusion: In the general practice setting in Toledo, Spain, from March 1, 2020 to September 1, 2022, with a majority of reinfections during 2022 coinciding with the predominance of omicron, the relative effectiveness of the COVID–19 booster against reinfections versus only 1 or 2 doses of vaccine was relatively low. However, our cohort was too small to allow precise determination of vaccine effectiveness.
Keywords: COVID–19 ; SARS–CoV–2; Reinfections; COVID–19 Vaccine; Vaccine Effectiveness; Breakthrough Infection; General Practice; Public Health.
The rapid development of multiple vaccines against the coronavirus disease 2019 (COVID–19 ) has been a triumph of biomedical research. However, the vaccine must face several problems, such as uneven distribution, vaccine hesitancy, decreased immunity, and the emergence of highly transmissible viral variants that partially escape antibodies [1]. Large–scale efficacy trials showed that COVID–19 vaccines reduced the risk of disease by more than 90% [2–3]. Likewise, the short–term efficacy of vaccines with respect to the severity of infection by the severe acute respiratory syndrome coronavirus (SARS–CoV–2) has been demonstrated [4].
However, on the other hand, there is growing scientific evidence showing that the protection generated through vaccination decreases over time, although it is restored with the inoculation of a booster dose. In addition, the decrease in immunity as a consequence of the new variants must be taken into account. Thus, it has been published that the risk of reinfection by COVID–19 is approximately 5% at three months, which increases to 50% at 17 months [5].
It has been reported that after several months, people with hybrid immunity were better protected against reinfection than uninfected people who had previously received two doses of the vaccine [6], but in any case, natural infection does not protect against contagion to new variants [10, 11]. Despite vaccinations, boosters, and natural immunity, the highly infectious omicron variant appears able to evade any protection it may have gained against SARS–CoV–2. The latest subvariants of omicron are causing reinfections to occur more frequently. The virus mutates more frequently than previously thought, and its mutations have been shown to be more infectious than previous strains [12,13].
After just two doses of the vaccine, when the omicron variant predominated, vaccine effectiveness against hospitalizations dropped from 71% within two months of vaccination to 54% within at least five months. The data also showed that the effectiveness of the vaccine decreased while the Delta variant was dominant. Among recipients of three doses during the time Delta was dominant, vaccine efficacy against COVID–19 –associated hospitalizations decreased from 96% within two months of vaccination to 76% at least months later [14]. Data have shown that the effectiveness of the vaccine in reducing the risk of hospitalization and admission to the ICU was greater after the booster inoculation than after the second dose, although it decreases over time [15].
In reality, vaccines are working remarkably well given the challenges of evolution, but because of the results of reinfection rates, experts stress the importance of booster doses; according to this, focusing on the primary vaccination schedule is no longer enough. Data have shown that the effectiveness of the vaccine in reducing the risk of hospitalization and admission to the ICU was greater after the booster inoculation than after the second dose, although it also decreased over time [15]. In this regard, mRNA vaccines have been reported to offer a similar degree of protection against Omicron's BA.1 and BA.2 subvariants, although again, protection against SARS–CoV–2 infection and symptomatic disease is diminished within a few months of booster dose [16].
However, many studies of post–vaccination and post–infection immunity have looked at a limited range of population subsets [17], and the consequences of reinfection at the individual level (severity of symptoms after the second infection) or at the population level (ability to spread of the virus) are not yet fully understood. In any case, reinfections might not be cause for alarm; Reinfections are also seen in many other respiratory viruses [18]. It is admitted that people need to get used to the idea of COVID–19 becoming a disease that they are likely to catch from time to time, just like the flu. So there is a strong possibility that COVID–19 will develop into a chronic viral infection for which you may or may not need to get an annual booster shot, although that is not yet known. SARS–CoV–2 will constantly mutate and have variants that may or may not be of different severity, with different transmissibility. As with the flu, annual boosters of the COVID vaccine will help protect against serious illness, but will not prevent a mild infection [12].
In summary, what do we currently know about the immune response to SARS–Cov–2 and the possibility of reinfection?:
In this scenario, one wonders if the booster vaccination provides advantages to prevent reinfection over only 1 or 2 doses of COVID–19 vaccine. Here we present a study that aims to compare the clinical–epidemiological characteristics of the cases of COVID–19 reinfection with vaccination (1 or 2 doses) with the cases of COVID–19 reinfection with booster.
An observational, longitudinal and prospective study of COVID–19 breakthrough infections in vaccinated people with vaccine booster was conducted from December 1, 2021 to February 28, 2022, in a general medicine office in Toledo, Spain, which has a list of 2,000 patients> 14 years of age (in Spain, the general practitioners [GPs] care for people > 14 years of age, except for exceptions requested by the child's family and accepted by the GP). The GPs in Spain work within the National Health System, which is public in nature, and are the gateway for all patients to the system, and each person is assigned a GP [19].
The objectives of the study were: A. To compare the cases of reinfections by COVID–19 in people vaccinated with a booster vaccine or 1 or 2 doses; And B. To assess the relative effectiveness of booster vaccination to prevent reinfection versus only 1 or 2 doses. Relative vaccine booster effectiveness to prevent reinfections was calculated as a percentage [20–23], as follows: 1– [Cases with vaccine booster shot / Cases with 1 or 2 doses, but without vaccine booster shot] × 100 [20–23].
The data sources and methods for this study were described previously [24–27]. In the current study, a larger series of reinfection cases is included, with a longer follow–up time from March 2020 to September 1, 2022, but the methodology remained unchanged from previous published studies. Below we repeat only some aspects to facilitate the understanding of this text. SARS–CoV–2 reinfection was conventionally defined as a documented infection occurring at least 90 days after a previous infection [28–30]. The diagnostic criteria for COVID–19, the definitions of vaccination with 1, 2 or 3 doses (booster) have been previously published for this study [24–27].
Collected variables were: Age and sex; Symptoms of COVID–19 in reinfection; Chronic diseases [31], classified according to the International Statistical Classification of Diseases and Health–Related Problems, ICD–10 Version: 2019 [32]; Patients with the presence of at least one chronic disease; Dates of COVID–19 reinfection; Social–occupancy class (according to the Registrar General's classification of occupations and social status code [33]; If they were Health Care Workers; Problems in the family context and low income household based on the genogram and in the experience of the GP for their continuity of care and knowledge of the family [34]; Ethnic minority [35]; Severity of the disease [36]; Vaccinated with 1 dose, with 2 doses, with booster, and not vaccinated against COVID–19.
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test.
From March 2020 to September 1, 2022, 47 cases of COVID–19 reinfection were included: 9 cases of COVID–19 without vaccination, 15 cases of COVID–19 reinfection with booster, and 23 cases of COVID–19 reinfection with vaccine (1or 2 doses), but with 25 infections (2 cases presented 2 reinfections: 2 women aged 17 and 19, with 2 and 1 dose of the vaccine, respectively) (Figure 1). The only statistically significant differences between COVID–19 reinfection with booster vs. with only 1 or 2 doses of vaccine, were that COVID–19 reinfection with booster were fewer women, more health care workers, fewer chronic diseases present, and more chronic diseases of the genitourinary group. There were no statistically significant differences in social, family, ethnic factors or year of reinfection. The majority of reinfections occurred during 2022, coinciding with the predominance of omicron. The vast majority of reinfections were symptomatic, all mild, and without statistically significant differences in their symptoms, although ENT symptoms clearly predominated in cases of COVID reinfection with booster (Tables 1–4). Relative vaccine booster effectiveness to prevent reinfections vs. only 1 or 2 doses, calculated as a percentage based on the formula: 1 – [COVID–19 cases incidence with vaccine Booster / COVID–19 cases incidence without vaccine Booster] × 100, was 40% (Table 5).
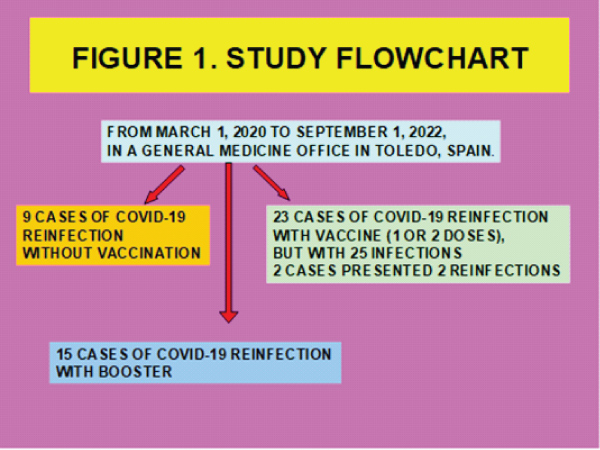
Figure 1: Study Flowchart.
Table 1: Variables in COVID–19 Reinfection with Booster Versus Without Booster (Only Vaccine 1 or 2 Doses).
Variables |
COVID–19 Reinfection with Booster N=15 |
COVID–19 Reinfection Without Booster (Only Vaccine 1 or 2 Doses) N=23 |
Statistical Significance |
> = 65 years |
1 (7) |
2 (9) |
Fisher exact test= 1. NS |
Women |
9 (60) |
21 (91) |
X2=5.353. P= .020686. Significant at p < .05. |
Health Care Workers |
6 (40) |
1 (4) |
X2 with Yates correction= 5.49. p= .019126. Significant at p < .05. |
Moderate–severe severity of primary infection |
2 (13) |
1 (4) |
Fisher exact test= 0.5501. NS |
Moderate–severe severity of reinfection |
0 |
0 |
Fisher exact test= 1. NS |
Chronic diseases presence |
6 (40) |
19 (83) |
X2= 7.3235. p= .006806. Significant at p < .05. |
Social–occupancy class of patients (people with some type of labor specialization) |
9 (60) |
7 (30) |
X2= 3.2555. p= .071183. NS |
Complex family/ Problems in the family context |
1 (7) |
2 (9) |
Fisher exact test= 1. NS |
Low income household |
1 (7) |
3 (13) |
Fisher exact test= 1. NS |
Ethnic minority |
3 (20) |
2 (9) |
Fisher exact test= 0.3649. NS |
( ): Denotes percentages; NS: Not significant |
|||
Table 2: Variables in COVID–19 Reinfection with Booster Versus Without Booster (Only Vaccine 1 or 2 Doses).
Variables |
COVID–19 Reinfection With Booster N=15 |
COVID–19 Reinfection Without Booster (Only Vaccine 1 or 2 Doses) N=23, with 25 Infections* |
Statistical Significance |
Symptomatic COVID–19 reinfection |
15 (100) |
23 (92) |
Fisher exact test= 0.5192 . NS |
Reinfección en 2020 |
0 |
1 (4) |
Fisher exact test= 1. NS |
Reinfección en 2021 |
2 (13) |
8 (32) |
X2 with Yates correction= 0.8889. p= .345779. NS |
Reinfección en 2022 |
13 (87) |
16 (64) |
X2 with Yates correction= 1.4127. p= .234601. NS |
( ): Denotes percentages; NS: Not significant; *Covid–19 reinfection without booster (only vaccine 1 or 2 doses) n=23 people; 25 infections: 2 cases presented 2 reinfections: 2 women aged 17 and 19, with 2 and 1 dose of the vaccine, respectively. The number of infections is used as denominator: N=25 |
|||
Table 3: Chronic Diseases in COVID–19 Reinfection with Booster Versus Without Booster (Only Vaccine 1 or 2 Doses).
Chronic Diseases* |
COVID–19 Reinfection With Booster N=15 |
COVID–19 Reinfection Without Booster (Only Vaccine 1 or 2 Doses) N=23 |
Statistical Significance |
–I Infectious |
0 |
0 |
Fisher exact test= 1. NS |
–II Neoplasms |
0 |
1 (2) |
Fisher exact test= 1. NS |
–III Diseases of the blood |
0 |
0 |
Fisher exact test= 1. NS |
–IV Endocrine |
5 (18) |
6 (14) |
X2 with Yates correction= 0.0458. p= .830463. NS |
–V Mental |
0 |
5 (11) |
Fisher exact test = 0.1489. NS |
–VI–VIII Nervous and Senses |
1 (4) |
5 (11) |
Fisher exact test = 0.3968. NS |
–IX Circulatory system |
1 (4) |
6 (14) |
Fisher exact test = 0.24. NS |
–X Respiratory system |
2 (7) |
9 (20) |
X2 with Yates correction= 1.2931. p= .255477. NS |
–XI Digestive system |
4 (15) |
2 (5) |
Fisher exact test= 0.1921. NS |
–XII Diseases of the skin |
1 (4) |
2 (5) |
Fisher exact test= 1. NS |
–XIII Musculo–skeletal |
4 (15) |
5 (11) |
X2 with Yates correction= 0.0032. p= .954609. NS |
–XIV Genitourinary |
9 (33) |
3 (7) |
X2 with Yates correction= 6.5944. p= .01023. Significant at p < .05. |
TOTAL chronic diseases* |
27 (100) |
44 (100) |
––– |
( ): Denotes percentages; NS: Not significant; *Patients could have more than one chronic disease. The percentages of chronic diseases are over the total of chronic diseases of symptomatic and asymptomatic patients |
|||
Table 4: Symptoms COVID–19 Reinfection with Booster Versus Without Booster (Only Vaccine 1 or 2 Doses).
Symptoms COVID–19 Reinfection* According to WHO, ICD–10 Groups |
COVID–19 Reinfection with Booster N=15 |
COVID–19 Reinfection Without Booster (Only Vaccine 1 or 2 Doses) N=23, With 25 Infections** |
Statistical Significance |
General (discomfort, asthenia, myalgia, fever, artralgias) |
21 (40) |
21 (40) |
X2= 0.0063. p= .936487. NS |
Respiratory (cough, dyspnea, chest pain) |
13 (25) |
16 (30) |
X2= 0.3535. p= .552147. NS |
ENT (anosmia / ageusia, odynophagia, rhinorrhea, pharyngeal dryness–mucus, epixtasis) |
16 (31) |
9 (17) |
X2= 2.7507. p= .09721. NS |
Digestive (anorexia, nausea / vomiting, diarrhea, abdominal pain) |
0 |
3 (6) |
Fisher exact test= 0.2429. NS |
Neurological (headache, dizziness, mental confusion –brain fog) |
2 (4) |
4 (7) |
X2= 0.8513. p= .356188. NS |
Psychiatric (anxiety, insomnia) |
0 |
0 |
Fisher exact test= 1. NS |
Skin (chilblains, flictenas, rash) |
0 |
0 |
Fisher exact test= 1. NS |
Total symptoms* |
52 (100) |
53 (100) |
––– |
( ): Denotes percentages; NS: Not significant; * Patients could have more than one symptom. The percentages are over the total of symptoms; **Covid–19 reinfection without booster (only vaccine 1 or 2 doses) N=2 people; 2 cases presented 2 reinfections: 2 women aged 17 and 19, with 2 and 1 dose of the vaccine, respectively. The number of infections is used as denominator: N=25 |
|||
Table 5: Relative Vaccine Booster Effectiveness to Prevent Reinfections Versus Vaccine ONLY 1 or 2 Doses.
Cases with Vaccine Booster Shot |
Gross Incidence Rate |
Cases Without Vaccine Booster Shot) (Only 1 or 2 Doses) |
Gross Incidence Rate |
|
15/40 |
37.50% |
25/40 |
62.50% |
|
Relative vaccine booster effectiveness to prevent reinfections vs. only 1 or 2 doses: [1 – (Cases with vaccine booster shot / Cases con 1 or 2 doses but without vaccine booster shot) x 100]= 40%. |
||||
Being fully vaccinated (meaning receiving a full dose of the vaccine and booster shots) remains the best way to protect against COVID–19: people who are vaccinated are less likely to get sick and much less likely to develop severe symptoms. Research has shown that having contracted and then recovered from COVID–19 adds additional protection. However, that protection isn't 100 percent effective, and its strength seems to wane over time. It is admitted that, even in a person who has already been infected, the vaccine can provide greater coverage of new variants and lessen or even eliminate symptoms if reinfected [37].
The main finding of our study is that we found a relative vaccine booster effectiveness vs. vaccine only 1 or 2 doses, against reinfection by COVID–19 (calculated as a percentage based on the formula: 1 – [COVID–19 cases incidence with vaccine Booster / COVID–19 cases incidence without vaccine Booster] × 100) relatively low of 40%. Other data are that the cases of COVID–19 reinfection with booster were fewer women, more health care workers (possibly because this group received the booster more frequently and is more exposed to infection). There were no differences in social, family, ethnic factors or year of reinfection. The majority of reinfections occurred during 2022, coinciding with the predominance of omicron. The vast majority of reinfections were symptomatic and all were mild, and without statistically significant differences in symptoms between cases with booster and cases with only 1 or 2 doses of vaccine, although ENT symptoms clearly predominated in cases of COVID–19 reinfection with booster.
It has been reported that among patients who had recovered from COVID–19, receiving at least one dose of the vaccine was associated with a significantly lower risk of recurrent infection, which is consistent with data showing strong immune responses to vaccination in previously infected persons [38, 39]. Other studies have reported that receiving more than one dose of the vaccine, in patients recovered from COVID–19, was not associated with greater effectiveness (40). Another study showed that among patients who had recovered from COVID–19, receiving one dose of the BNT162b2 vaccine was associated with an 82% lower risk of recurrent SARS–CoV–2 infection among those between 16 and 64 years of age and 60% lower risk among those over 65. No substantial difference in risk of reinfection was found for two doses of vaccine compared to one dose [8].
On the other hand, it has been published that two doses of the BNT162b2 vaccine were associated with high short–term protection against SARS–CoV–2 infection; this protection diminished considerably after 6 months. Immunity acquired by vaccination–enhanced infection remained high for more than 1 year after infection [4].
According to experts, infections or reinfections by variants of COVID–19 and associated hospitalizations are preventable with booster doses. The Centers for Disease Control and Prevention say that among people with prior SARS–CoV–2 infection, get a dose of mRNA vaccine provided protection against subsequent hospitalization for COVID–19 reinfection. The highest level of protection was conferred by a booster dose, with similar vaccine effectiveness during the delta and omicron predominant periods (approximately 60%–70%). In contrast, the vaccine effectiveness of 1 or 2 doses decreased from 50% to 60% during the delta predominant period to approximately 35% during the omicron predominant period [13]. Our study includes all the period of the pandemic, from March 2020, although the vast majority of reinfections occurred at the end of 2021 and during 2022, coinciding with the increase in omicron. Considering all this period, relative vaccine booster effectiveness to prevent reinfections vs. only 1 or 2 vaccine doses, was low (40%), but without any serious illness.
Surveillance data collected in the UK reveal that less than 20% symptomatic COVID–19 vaccine effectiveness after 25 weeks or more after a second dose, but increases to approximately 70% in 2–4 weeks after third dose [16]. Other studies show that protection against serious illness remained 68% or higher for at least 7 months, even in people who had only received two doses of the vaccine, and spiked to more than 80% after a booster dose [16]. During the delta wave, two doses of COVID–19 vaccine were found to be about 47% effective against hospitalization due to reinfection and a booster dose was more than 57% effective. And during the wave of omicron, the two–dose series was about 34% effective and the booster dose about 68% effective against hospitalization due to reinfection [40]. Multiple studies have shown that neutralizing antibodies induced by all primary vaccine regimens show little cross–reactivity with omicron, but that boosting leads to a substantial increase in neutralizing antibodies to omicron. However, these increased neutralizing antibody titters, as well as clinical effectiveness, have been shown to wane by 4 months after a third mRNA immunization [1, 14, 41].
In summary, growing concerns about the long–term efficacy of COVID–19 booster vaccines have been exacerbated by the emergence of omicron subvariants. Experts think that boosters and previous infections can still help prevent more serious cases of COVID–19. However, the protective effectiveness would not be strong enough to prevent initial infection or mild illness. There is a possibility that the COVID–19 virus could develop into a chronic viral infection. Therefore, it will be necessary to receive an annual booster of the vaccine. The COVID–19 pandemic appears to be transitioning from an acute phase to an endemic phase. Current COVID–19 vaccines are less effective at blocking infection with the omicron variant than they are at blocking infection with earlier variants, but protection against severe disease is largely maintained. The primary goal of COVID–19 vaccines should be to provide long–term protection against serious illness, hospitalization, and death (1). Against this background, expert opinion on the benefits of frequent booster remains divided. Boosting every 4 to 6 months to maintain high serum neutralizing antibody titters may not be a practical or desirable long–term strategy. Experts recommend them for people who are at high risk for severe illness. For those without risk factors, experts advise waiting, especially if they have had COVID–19 before. Frequent booster recommendations may also distract from the critical goal of vaccinating the large number of unvaccinated people around the world and may further exacerbate global health inequalities [1, 12].
The study has certain limitations that must be taken into account:
In our context, considering the data from the entire time of the COVID–19 pandemic, we found a relatively low vaccine booster effectiveness to prevent reinfections of 40% vs. only 1 or 2 doses of vaccine, although without any serious cases. However, our cohort was too small to allow precise determination of vaccine effectiveness. The effectiveness of the booster against only 1 or 2 doses of vaccine seems not to be strong enough to prevent reinfection with mild disease, being less effective in blocking infection with the omicron variant than with previous variants, although protection against severe disease is largely maintained. Possibly boosters should be recommended for people who are at high risk of severe disease.
None.
Author declares there is no Conflict of interest.