Background: Although there is disagreement about the definition and clinical relevance of the placebo effect, the use of inert or non-indicated medication has been common throughout the history of medicine. There is increasing evidence that placebos are effective in clinical practice. However, knowledge of the epidemiology of the placebo effect is poorly developed.
Aim: To explore, describe and discuss the topic of epidemiology of placebo effect, in a broad way, considering multiple factors from a theoretical and contextual point of view and its impact on epidemiology.
Methods: This article should be considered as a personal point of view, based on the author's experience, plus an non-systematic or opportunistic search for information.
Results: Scientific evidence has shown that the placebo effect exists: it is a true biopsychosocial phenomenon produced by the context in which an intervention is carried out. The placebo is viewed from a different perspective in clinical trials or in clinical practice: 1. the placebo effect occurs in 100% of treatments in clinical practice; placebo effect is a part of all regular treatment. It's not drug or placebo; it’s drug and placebo. On the other hand, many doctors admit to regularly prescribing placebos, but there are marked differences on the frequency of their use, because of the different definition criteria, but with a high prevalence that is greater than 50% in the treatment courses; 2. Numerous clinical trials have calculated the magnitude or rate of the placebo effect in different clinical conditions. The magnitude of the placebo effect ranges from an average rate of 35% in classic reviews, 62% in neuropathic pain, 40% in fibromyalgia and restless legs syndrome, 25% in patients with schizophrenia and 68% in unipolar depression.
Conclusion: It can be said that the placebo response is a complex phenomenon that has many variables; there is no single placebo effect, but rather many effects with different mechanisms, in different medical conditions, and different therapeutic interventions.
Key Words: Placebo Effect; Specific and Non-Specific Treatment Effects; Clinical Research; Controlled Clinical Trials; Epidemiology
Placebos are substitutes for drugs or active interventions that can improve symptoms in patients when prescribed or performed by a physician and for a patient and their effect cannot be explained by the drug itself or the intervention itself. In research studies and presumably in clinical routine as well, placebo effects contribute substantially to drug efficacy. Although this is a field whose evidence is still developing, current knowledge is growing by approximately 10,000 publications per year on placebo-controlled studies, and almost 100 articles on the placebo effect itself (1).
The term placebo has been used since at least the 18th century to describe innocuous, indulgent treatments; But since the second half of the 20th century, with the development of the randomized clinical trial (RCT), which requires the comparison of a study drug with an identical-looking placebo, interest in placebo and its effects has intensified.
An example of clinical trials performed by examining placebo effect (PE) would be the following:
Placebo has been defined in many ways; for example, placebo can be defined as any therapy or component of therapy that is used for its non-specific psychological or psychophysiological effect, or for its presumed specific effect, but is without specific activity for the condition being treated (5); but this definition presents the problem of how specific and nonspecific effects are defined.
On the other hand, understand the PE as the difference in outcome between a placebo treated group and an untreated control group in an unbiased experiment, reflects the impossibility of defining the PE in a single case, where biases of various types cannot be excluded. In summary, it can be said that a PE is the non-specific effects of the treatment. Therefore it be said that the PE is defined as the changes produced by placebos (6, 7). That is, simplifying, placebo is defined as an inert substance that provokes perceived benefits (8-10).
There are recovery mechanisms of the disease that are more complex than homeostasis. Among these is the PE. They are true social, cultural and psychobiological responses that can significantly modify the overall outcome of the treatment. The effects of placebo occur frequently and are clinically significant, but are not recognized despite the comprehensive framework of general medicine (7). The experts agreed that it is crucial to distinguish between placebo responses versus PE. The placebo response includes all health changes that result after administration of an inactive treatment (i.e., differences in symptoms before and after treatment), thus including natural history and regression to the mean.
The PE refers to the changes specifically attributable to placebo mechanisms, including the neurobiological and psychological mechanisms of expectancies. These mechanisms are shaped, for example, by verbal instruction, or nonverbal or situational cues that affect treatment expectancies. Importantly, placebos not only have effects during the prescription of placebo pills, but they can also substantially modulate the efficacy and tolerability of active pharmacological or other medical treatment (10).
The obvious ways of doing medicine actually depend on a hidden world view, a framework of unexamined assumptions that keeps our thinking in place: mind-body dualism, bias towards reductionism, etc.). A common assumption is that placebos are "stuff" that tricks us into feeling better. But in reality, most of the outcome of any treatment has to do with factors that are anything but biological; even apparently unequivocal clinical facts are actually dependent on culture and custom. Health and health care are linked to culture (11, 12).
The placebo does not act purely by suggestion. The PE is not only a psychological effect or something that depends solely on our attitude or our perception. PE is psychobiological events imputable to the therapeutic context. Placebo represents complex and distinct psycho neurobiological phenomena in which behavioral and neurophysiologic modifications occur together with the application of a treatment (13). PE rely on complex neurobiologic mechanisms involving neurotransmitters (eg, endorphins, cannabinoids, and dopamine) and activation of specific, quantifiable, and relevant areas of the brain (eg, prefrontal cortex, anterior insula, rostral anterior cingulate cortex, and amygdala) in placebo analgesia (14).
It has also been reported that these changes seem to depend on a family of neurotransmitters called catecholamines -to which adrenaline, noradrenaline and dopamine belong- implicated among other factors in the stress response, and certain mutations have been discovered in an enzyme called catecholmethyltransferase (which alter the levels of these neurotransmitters) that can predict whether a patient will have a greater or lesser PE, demonstrating that this effect may have a genetic basis (15-22).
A plethora of potential mechanisms of the PE exist: operant conditioning, expectancy effects, guilt reduction, transference, suggestion, persuasion, role demands, hope, faith, labelling, selective symptoms monitoring, misattribution, cognitive dissonance, control theory, anxiety reduction, expectancy effects, endorphin release and a variety of design and measurement artefacts (7, 23-25). There is increasing evidence that placebos are effective in clinical practice. However, knowledge of the epidemiology of the PE is poorly developed. In this scenario, this article aims to reflect and conceptualize the fundamental epidemiological elements of PE and its practical applications.
The comments in this article should be considered as a personal point of view, based on the author's experience. It is therefore an argumentative writing and critical thinking, plus an unsystematic or opportunistic search for information. The search for information was based on a non-systematic review considering the bibliographic references of selected articles, reviews of books related to the topic and opportunistic searches on the Internet. The keywords “placebo” and "placebo effect" were mainly used and in Google search engines, as well as in Google Scholar, Pubmed and SciELO. This non-systematic review was carried out, which aimed to explore, describe and discuss the topic of epidemiology of PE, in a broad way, considering multiple factors from a theoretical and contextual point of view and its impact on epidemiology.
Placebo is viewed from a different perspective depending on whether it is used in clinical trials or in clinical practice. TABLE 1 shows some aspects of its distribution, frequency and determining factors.
Table 1: Epidemiology of Placebo effect: Distribution, Frequency and Determining Factors.
FACTORS |
CONCEPT |
1. Placebo effect is context-dependent and part of effective treatment |
Placebo effects are the effect of patients positive expectations concerning their state of health. These effects occur in many clinical contexts, including treatment with an active agent or a placebo in clinical practice or in a clinical trial, the informed-consent process, the provision of information about medical treatments, and public health campaigns. |
2. Placebo effect in clinical practice |
Between 45% and 97% of doctors admit to having used a placebo |
3. Placebo effect in clinical trials |
The benefit of drugs attributed to the placebo effect reaches 62% in neuropathic pain and 40% in fibromyalgia and restless legs syndrome, 25% in patients with schizophrenia5 and 68% in unipolar depression |
4. Epidemiological factors that determine the size of the placebo effect |
Placebo responses are changes in patients' symptoms attributable to their participation in the therapeutic encounter, with its rituals, symbols, and interactions; this multitude of signals inherent to any intervention are perceived and interpreted by patients, generating positive or negative expectations |
5. The placebo effect is not a pill, it is a process |
Placebos are a contextual processes |
6. Factors that can create false impressions of placebo effect |
The fluctuation of symptoms or disease course and natural improvement of a disease, etc. |
Placebo Effect is Context-Dependent and part of Effective Treatment
PE refers to a patient's symptom improvement when receiving an inert agent or procedure. Placebos have been associated not only with patient comfort but also with beneficial responses at least since the 18th century (26, 27). Robust empirical evidence now demonstrates that PE is significant and measurable for many conditions (e.g., pain, depression, Parkinson's disease, fatigue, allergies, and immune deficiencies) (10, 22). Each treatment in medicine determines, at the same time, biological, psychological and social effects, these can be specific and contextual (or nonspecific) effects, which interact with each other (7). Conventional medical research routinely assumes that specific and nonspecific effects are simply additive and do not interact (28, 29). But that assumption is false. PE is apart of effective treatment. It's not drug or placebo; It's drug and placebo (10).
The question of the placebo raises the issue of social reality rather than ontology, since the content of the placebo is often anticipated to be 'believe'. This extended anthropological notion of placebo includes "pill and procedure and its context," and thus multiple social realities rather than universal and exclusive ontologies help us accept the diversity of healing. To explore the deep layers of the PE, we need knowledge of the physical, cultural, social, and economic context. On the other hand, a social psychophysiological approach helps to reintegrate the more subtle social and cultural influences into the naturalistic framework (11, 30).
Placebo Effect in Clinical Practice
Placebo is viewed from a different perspective depending on whether it is used in clinical trials or in clinical practice. When there are no ethical impediments, the placebo-controlled clinical trial is the best method to demonstrate the efficacy of a drug. Health professionals report using placebos at markedly different frequencies and this is highly influenced by how placebos are defined in the studies (31).
The use of placebo (pure or impure) is common in clinical practice, as indicated by surveys carried out in different countries. In them, between 45% and 97% of doctors acknowledge having used placebos, in the vast majority of cases impure placebos such as antibiotics for viral infections, analgesics, drugs at subtherapeutic doses or vitamins. In the US, 55% of internists and rheumatologists reported using placebos; in the UK, 77% of primary care doctors reported that they used placebos at least once per week, while 86% of primary care doctors in Denmark admitted that they had used placebos at least once within the last year; 86% reported to have used placebo interventions at least once, and 48% to have used placebo interventions more than ten times, within the last year. The most frequently cited reasons have been unjustified demand for medication by the patient, calming him or the exhaustion of other therapeutic options (10, 32-39).
Variation in the ways that patients respond to treatments and experience symptoms is partly attributable to PE. The frequency and intensity of PE in clinical practice are difficult to determine, and the range of effects in experimental settings is wide (22). It is generally assumed that the administration of an inert pill can have therapeutic effects in one third or more of all patients in a variety of diseases. But in the literature the magnitude and frequency of the PE may be exaggerated, or wrong. The reasons for the inconsistency of the epidemiological data of the PE are due to documentation errors, methodological and conceptual errors; In addition, large variations in the data between different contexts can be assumed, because of the PE is a context-dependent effect (5).
Placebo Effect in Clinical Trials
Henry Beecher (26) was one of the first researchers to note the phenomenon of the PE. In his landmark article he reviewed 15 placebo-controlled trials and concluded that, on average, the magnitude of the placebo was 35%, but many methodological errors were not taken into account. The observed treatment effect in treatment group is made up of two components: the direct response to provision of the active therapeutic drug and non-specific treatment effects not directly ascribed to the active treatment. These non-specific effects include the PE and the natural disease history.
It is generally accepted that the PE represents the patient's response to intervention, including the patient's response to a therapeutic ritual, subsequent response to observation and assessment, and response to the patient-doctor interaction. No doubt there is a complex relationship between these three components. The PE can be observed in any medical encounter and not solely in clinical trials that incorporate a placebo treatment group. It is possible that the provision of any therapeutic regimen will elicit a PE, but it may, however, be enhanced in clinical trials, when compared with routine clinical practice, because trial participants typically receive additional care and attention. Although the PE is generally held to exist, debate exists as to the magnitude of the treatment effect it represents (40).
PE has been measured in thousands of medical experiments. Over the last decades, numerous studies have calculated the magnitude of the PE in different clinical conditions. Until recently, most estimates have been based on the results obtained in the placebo groups of RCTs that are carried out to compare the efficacy of drugs. Placebo responses in these studies are difficult to interpret because they may include external factors such as spontaneous remission or regression to the mean. However, these data provide a good estimate of patient improvement without the benefit of the study drug. More recently, studies designed directly to investigate the PE have shown that it primarily affects self-reported symptoms and global outcomes of improvement (41).
A systematic review including 202 RCTs, with a no treatment control group and investigating 60 clinical conditions, found no important clinical effects of placebo interventions. Statistically significant differences were found in pain disorders, nausea, asthma and phobia. Significant variations in the PE were found, which the authors explain by different study designs, the type of placebo used, and whether or not patients were informed that the study included placebo (42).
In general, subjective symptoms unrelated to underlying organic diseases, such as pain, irritable bowel syndrome, or depressive symptomatology, are more likely to respond to the PE, although it has also been shown to be beneficial in diseases such as Parkinson's, asthma, or ulcers of duodenum (43). Systematic reviews show that the benefit of medications attributed to PE reaches 62% in neuropathic pain and 40% in fibromyalgia and restless legs syndrome. In the psychiatric field, PE is lower in psychotic disorders than in neurotic disorders, reporting an average rate of 25% in patients with schizophrenia and 68% in unipolar depression (FIGURE 1). The transversality of the phenomenon reaches the surgical field, observing that the removal of degenerated cartilage with knee arthroscopy is not more effective for the management of chronic pain when compared with placebo surgery and that placebo surgery in patients with Parkinson's is capable of relieving some symptoms for prolonged periods of time (22). In many double-blind clinical trials of treatments for pain or psychiatric disorders, for example, the responses to placebo are similar to the responses to active treatment (22).
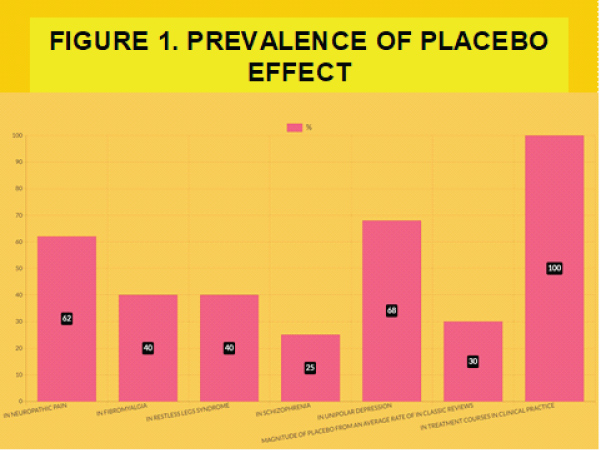
Figure 1: Prevalence De Placebo Effect
Epidemiological Factors that Determine the size of the Placebo Effect
Placebo interventions vary in strength depending on many factors. The concept of “total drug effect” whereby the overall effect of a drug on an individual usually depends on a number of different factors in addition to (or separate from) its pharmacological action:
In this way, the PE would be the total drug effect, but without the pharmacological presence of any drug (5, 20, 44, 45).
The relationship of trust may be sufficient to improve symptoms of stress or anxiety, so that the effect attributed to any prescribed medication may be due to that relationship. It is about "the effect of the doctor himself as a drug". The medicine most frequently used by general practitioners is the doctor himself. Consequently, the doctor himself should be considered as a drug, that is, that the concepts of pharmacology, such as overdoses, allergic reactions, side effects, etc., can be applied to the interaction between doctor and patient. Both, doctor and patient, are modified: one towards the other and vice versa (46-49).
The therapeutic outcome seems to be impacted by rituals around a clinical encounter and by the doctor patient communication and relation. A warm, friendly and empathic attitude is crucial in the first contact with the practice and during the consultation as it influences the patient's perceived outcome. The context of the doctor-patient interplay matters, and placebo research provides strong evidence for this link. The therapeutic context induces biomedical processes in the patient's brain that may enhance or reduce the effects of chosen interventions. The context thus works as a drug, with real effects and side effects (10, 45, 50, 51).
Table 2: Epidemiology Factors that Determine the size of the Placebo Effect.
FACTORS |
CONCEPT |
Nature of intervention |
Surgery seems to be associated with extremely powerful placebo effects. An injection causes a stronger placebo effect than a tablet. Two tablets work better than one, capsules are stronger than tablets, and larger pills produce greater reactions. Red, yellow, and orange are associated with a stimulant effect, while blue and green are related to a tranquilizing effect |
Therapist |
Certain characteristics of the therapist induce stronger than average placebo responses: the status of professionals, empathy, warmth and understanding, Also, the therapist´s expectations are of critical importance |
Extended doctor-patient relationship (continuity of care) |
Although hard evidence is scarce, it seems conceivable that an extended doctor-patient relationship (continuity of care) might lead to stronger placebo effects than a short encounter. The time factor might work by increasing trust, expectation, etc. |
Patient |
The personality, the anxiety, the confidence in the doctors who treat him, his beliefs, the expectations deposited in the treatment. The simple fact of going to the doctor and feeling cared for constitutes, to a certain extent, a placebo effect for the patient. |
Nature of the complaint |
The type of disease, severity, intensity and its natural course |
Therapeutic setting |
Modern medicine is not culturally homogeneous, and the consulting rooms of doctors from different backgrounds often utilize very different symbols to create the right atmosphere. A formal clinical setting is more effective than an informal one. |
The placebo effect is not a pill, it is a process
The dominant construct of the "placebo pill" informs an incomplete understanding of placebos. The less-prevalent construct of the ‘treatment process’ frames placebos as potentially viable within modern evidence-based medicine (31, 56).
Factors that can create false impressions of placebo effect
When we administer a drug or intervention, there are many variables that can influence the clinical improvement of a patient. But, it must assess other phenomena that act as biases. These phenomena can confuse us and attribute responses to the PE that are not its own. Many factors and mistakes were found that create illusions of therapeutic PE (5, 20, 57, 58).
Table 2: Factors that can Create false Impressions of Placebo Effect.
FACTORS |
CONCEPT |
Natural, spontaneous improvement of a disease |
Many patients with mild diseases improve spontaneously |
Spontaneous fluctuation of symptoms or disease course |
Chronic diseases can have fluctuation of symptoms or of their course |
Regression to the mean |
Both fluctuation of symptoms or disease course and natural improvement of a disease are special forms of a regression to the mean, which always has to be considered when observations are started with values strongly deviating from the norm. In this situation subsequent observations are statistically more likely to measure more relatively normal ("improved") values than to measures more extreme values. Patients tend to consult doctors, because patients generally look for medical help when their symptoms are at a peak; In this situations symptoms will statistically improve rather than deteriorate |
Additional treatment. |
In many trials the patients received additional effective treatment. Por ejemplo, en el conditional switching of treatment: this kind of patient selection creates the illusion of effective placebo therapies |
Answer of politeness and experimental subordination |
Polite answer means that patients report improvement just to please the doctor, whereas in fact nothing has improved. A similar phenomenon is what is called "experimental subordination." This means that in an experiment subjects say what they think is expected of them, rather than they really experience |
Conditional answers |
It difficult to differentiate therapeutic placebo effects from conditioned effects. Conditioning is the basic constituent of placebo effects. However, conditioned effects need specifyc presuppositions: first a specific unconditioned stimulus and second a specific setting. Clinical experience contradicts the assumption that healing can be conditioned. Episodes of chronic disease are usually more difficult to treat than the acute or first manifestation of an illness, even if this first manifestation has been treated successfully, and classical conditioning predict just the opposite; moreover, there are many severe symptoms that are treated effectively by regular and repeated drug administration, and when such regular treatments are interrupted a rapid deterioration of patients is observed in practice |
Misquotations and uncritical reporting of anecdotes |
Wrong quotations are common in the placebo literature, or the number of treated patients is exaggerated and alters the data percentages. On the other hand, it is necessary to differentiate between genuine placebos and pseudoplacebos: the former predominate in clinical studies, while the pseudo-placebos prevail in "alternative" practical therapy. |
Although there is some disagreement about the definition and clinical relevance of placebo treatments, the use of inert or non-indicated medication has been common throughout the history of medicine. Today, the placebo is used primarily in research and in the study of the placebo phenomenon itself, and continues to be used in clinical practice as well. Scientific evidence has shown that the PE exists. It is an authentic biopsychosocial phenomenon produced by the context in which an intervention is carried out. Placebo is viewed from a different perspective depending on whether it is used in clinical trials or in clinical practice. PE occurs in 100% of the treatments. PE is apart of effective treatment. It's not drug or placebo; it's a drug and a placebo. On the other hand, many doctors admit to regularly prescribing placebos, but there are marked differences in the frequency of the use of placebos, in relation to the different definition criteria, but a high prevalence of the deliberate use of pure and impure placebos is admitted, which is higher 50% and probably close to 100% of treatment courses. Numerous clinical trials have calculated the magnitude or rate of the PE in different clinical conditions. In general, the PE has been shown to mainly affect self-reported symptoms and overall improvement results, being more likely in subjective symptoms not related to underlying organic diseases, such as pain or irritable bowel syndrome, but also in diseases such as Parkinson's, asthma or duodenal ulcer. Although placebo responses can be difficult to interpret, the magnitude of the placebo ranges from an average rate of 35% in classic reviews, with 62% in neuropathic pain, 40% in fibromyalgia and restless legs syndrome, 25% in patients with schizophrenia and 68% in unipolar depression. There is no single PE, but rather many effects with different mechanisms, in different medical conditions, and different therapeutic interventions.