Public Health is the care and promotion of health applied to the entire population. But public health should not be considered as something apart from the health of each individual and general medical care. Numerous social factors have a powerful influence on public health, which is why it is necessary to consider it from a comprehensive perspective. However, comprehensiveness is a principle that is difficult to implement in its dimensions and the role of the relational, community, and social is forgotten. Furthermore, Public health and general medicine are often conceived as two entities providing different services within the health system, and appear as separate disciplines, which are conceptualized, organized and financed as two distinct entities. Thus, it is important to reflect on the conceptual links between individual health and community health; that is, between public health and general medicine. General medicine is a public health tool, and the working instrument of general medicine is the biopsychosocial model. The concepts of comprehensiveness and biopsychosocial approach are those that give importance to general medicine as a basic tool of Public Health. The incorporation of a biopsychosocial perspective in general medicine results in a strengthening of the public health of the population. It is suggested to give more importance to the role of the general practitioner as a public health doctor, emphasizing the comprehensiveness of their work that allows the construction of scenarios for the health and life of communities.
Key Words: Public Health; General Practice; Biopsychosocial; comprehensiveness; Theoretical framework
The coronavirus disease 2019 (covid-19) pandemic has generated great awareness of Public Health and its important role in maintaining the health of the population. for both the public and the medical community. It is widely recognized that prior to the COVID-19 outbreak, medicine and public health practices often operated in separate silos (1).
Public Health is the care and promotion of health applied to the entire population, or to a precise group of the population. But, public health should not be considered as something separate, since it is closely related to the health of each one, medical attention and medical care. However, the links between individual health and community health have not been clearly conceptualized; that is, between public health and general medicine. The developments of integrated health care systems in which public health and individual health are treated equally have been advocated. Contrary to what happened in the past, when public health was mainly concerned with contagious diseases and sanitation, today public health analyzes a whole range of health determinants and focuses on promoting health and adopting preventive measures. Many social factors strongly influence public health, which is why it is necessary to consider it from a general perspective. In addition to communicable diseases and health, such an approach should include the social determinants of health, noncommunicable diseases, and lifestyles (2-4).
From the above, it can be extrapolated that comprehensiveness is one of the doctrinal principles of the Health Policy/Public Health. But, it is considered that comprehensiveness is a principle that is difficult to implement in its dimensions (5). In addition, many epidemiological and public health studies evaluate risks and protective factors focusing mainly on the individual, while theoretical frameworks emphasize the role of the relational, community, and social (6).
In 1977 Engel, from the University of Rochester, proposed a paradigm capable of scientifically including the human domain in the experience of illness: the biopsychosocial model. This model is derived from general systems theory, and emphasizes the need to consider psychological and social components in health care (7-9).
In Spain, although general medicine (Family and Community Medicine) was born under the patronage of tertiary hospitals, its development as a specialty (and much of its specific identity) is due to Public Health. The meaning of daily work is provided by the approach, the vision of the public health worker (10). General medicine as a component of Primary Care, has as its fundamental purpose to improve the level of health of the community through a comprehensive practice (prevention, recovery, rehabilitation and health promotion). In other words, general medicine is an instrument of Public Health. The purpose of general medicine is to improve public health (10, 11).
General medicine could be defined as the care level of provision of "integrated" and accessible services, where the vast majority of personal care needs are met, developing a continuous partnership with patients and working within the family and the community. Comprehensiveness is one of the four basic characteristics of family medicine, along with accessibility, coordination, and continuity or longitudinality (12, 13). General medicine provides comprehensive health services, which include the promotion of health, prevention of morbidity, curative care and terminal care, integrated and coordinated according to the needs of each patient (14). The practice of general medicine connects medicine with the community more than any other medical specialty. It can provide more intelligence on population health than any other medical source. Information on emerging epidemics, the impact of environmental hazards, and the consequences of changes in the social role and economic status of a community are available through the intelligent awareness and observation of general practitioners (GPs) (15). General medicine is defined in terms of relationships, which makes it unique in the main fields of clinical medicine (16). What characterizes and marks the difference in the work of the GP is the systemic approach (17, 18).
However, public health and general medicine are often conceived as two entities providing complementary services within the health system, and they appear as different and separate disciplines. Despite the fact that public health and general medicine are often conceptualized, organized, and funded as two separate entities, there is an emerging consensus that strengthening general medicine can support some public health functions and that public health can, in turn, improve the provision of general medical services to the entire population (19).
In this scenario, the objective of this article is to reflect on the natural affinities and common concepts between general practice and public health practice to use them as bridges to strengthen links.
In this article, we show a personal opinion, reflecting on the practice of the general practitioner as a public health tool. We carry out an exercise of rethinking the meaning of words as hackneyed as comprehensiveness and biopsychosocial model, critically evaluating and summarizing some evidence in a non-systematic or opportunistic references search, considering the bibliographical references of selected articles, basic and seminal book reviews related to the subject and opportunistic searches on the Internet about these concepts and their application or impact on public health.
To apply Public Health principles in addressing the needs of the local population, one must understand the unique characteristics of general medicine in this community. Knowledge of the community from general medicine allows GPs to interact dynamically with members of the community, often through the patients served in a continuing care, and create a lasting positive impact on the population/community (16, 20 -22).
Community health is the collective well-being of community members. In addition to living in the same neighborhood or region, these populations often share health characteristics, ethnicities, and socioeconomic conditions. For example, some low-income communities may experience high rates of obesity due to the limited availability of nutritious foods in local supermarkets. In addition, a population could be exposed to contaminants from a nearby plant or waste facility. Also, there may be disparities in community health levels; for example rural populations, populations exposed to higher levels of poverty, homelessness, substance abuse and other risk factors. Public health professionals and GPs identify how variables related to socioeconomic status, such as income levels, nutrition, crime, and transportation resources, affect people. They also determine how the community's medical and educational resources contribute to residents' lifestyles and what improvements are needed. The goal of the GP as a community doctor is to offer comprehensive services to patients and communities. GPs form strong ties with patients and citizens, as well as with social service providers and specialty health care providers in the area (16).
The comprehensiveness of the GP's work reflects the uniqueness and unity or integrity of human beings and their environment, and the concept refers to the General Systems Theory (23-26). The structure of systems is defined by the way in which the elements of a system are interconnected or communicated. Communication is the foundation of all social life. Communication is not a simple and linear process, but a complex and circular one. Various population groups have issues that require comprehensiveness as the basis of their health care strategies. For example, mental health, health of indigenous populations or women's health (27).
The general theory of systems states that the elements of an organized set (for example, members of a family, members of a group...) are related to each other in such a way that influencing one of the elements necessarily means influencing all of them. The healthcare-patient relationship is actually quadrangular (a matrix with the participation of four teams): GP-patient-family-context. GP is in contact with the patient for a few minutes, but the rest of the timepatient relates to his family and to his community context. Therefore, the family and the context must be taken into account as essential elements for the treatment (hygienic measures, diets, taking drugs, exercise or rest, etc.) (17, 28-32).
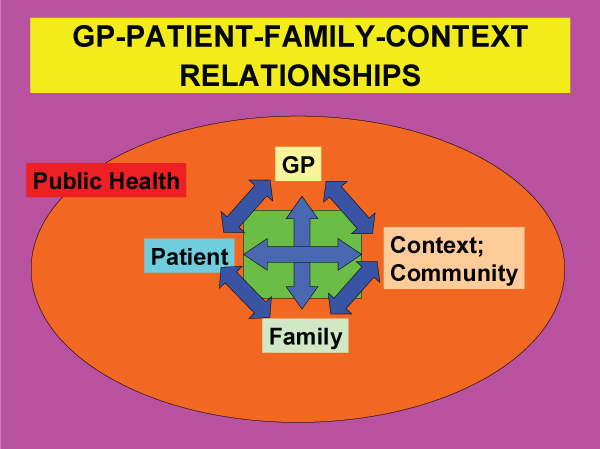
Figure 1: GP-Patient-Family-Context Relationship.
The GP is also related to the family: the degree of GP-patient cooperation is related to the degree of healthcare-family cooperation. The more complex the problem to be addressed the greater the need to work with the family group (13, 33). The family and the community are more than a group of individuals, since within them there is a set of stable interaction patterns that determine the behavior of the individuals that comprise it. Conceiving the family/community as a system helps to understand individual symptoms that may have a function within group dynamics. The persistence of symptoms may indicate a difficulty on the part of the family to adapt to a certain situation of change or to solve a certain conflict. At its core, systems thinking are endeavours to see how things are connected to each other within some notion of a whole entity (34).
Comprehensiveness implies understanding the patient, inserted in different contexts, from biopsychosocial, cultural and spiritual dimensions, focused on individual needs (12, 35-38). For theGP biopsychosocial approach skills are crucial. The GP should be able at the same time to have a scientific, interactive and simultaneous approach to each problem from biomedical, psychological, and social perspectives, and should be able to combine these perspectives in a panoramic view to achieve a complete understanding. GPs know that the elements of the patient's personality and their social relationships are of great importance in the disease, and these elements are as obvious and necessary as the biomedical aspects. The characteristic of family medicine is the understanding of the patient and her illness based not only on symptoms and signs, but also on the psychological and social factors that relate the patient to her context (39).
Biopsichosocial model identifies biological, psychological, and social factors as ever-present elements with interrelated influences on health and disease. If the application of scientific methodology discovers and allows the conclusion that the so-called social factors participate in some health process -in the origin, in the course, etc.- there is no reason to consider their importance less in relation to with that of other participating factors (for example, biologics factors), nor to assign them secondary or distant positions. In biopsichosocial model, the onset, diagnosis, course, prognosis, and treatment of disease are better understood by involving all 3 levels of analysis. biopsichosocial model is therefore a theoretical framework from which to view the disease. Nature is organized as a hierarchical unit that reflects a continuum of complexity: from small and uncomplicated to large and complex. Each unit represents a system with its own qualities, organization, and study methods that are appropriate to that system. Thus, the methodology for studying cell metabolism is totally different from the methodology for evaluating dysfunctional patterns of interaction in families with chronic diseases. Each system can only be fully characterized by understanding the larger system of which it is a part. In addition, psychological and social factors can influence and be influenced by the pathophysiological process (40, 41).
This article brings up the gap between public health and medical care. Much has been written about this divide and its consequences, but these efforts have been frustrated. The biopsychosocial model is put forward to better understand the impact of psychosocial factors on health and to stimulate greater interest of medical theory and practice in a more holistic approach. General medicine is a Public Health tool, and the working instrument of general medicine is the biopsychosocial model. In other words, the concepts of comprehensiveness and biopsychosocial approach are what give importance to general medicine as a basic tool of Public Health. The incorporation of a biopsychosocial perspective in general medicine results in a strengthening of the public health of the population. But this vision on the biopsychosocial model is still threatened by biomedical reductionism and does not resolve the dilemma between public health and general medicine. It is suggested to give more importance to the role of the general practitioner as a public health doctor, emphasizing the comprehensiveness of their work that allows the construction of scenarios for the health and life of communities.
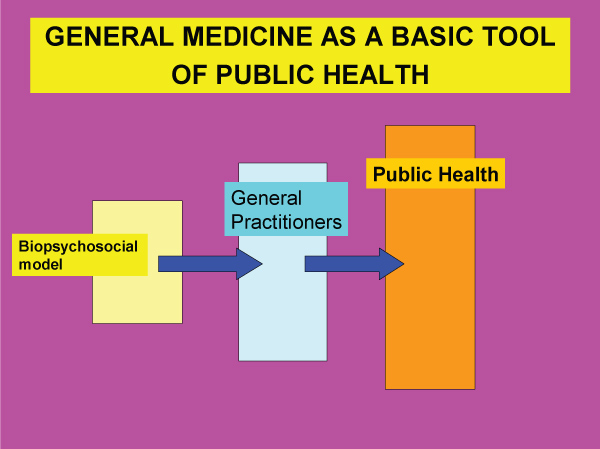
Figure 2: General Medicine as a Basic Tool of Public Health.