Sense of healing / health problem resolution is qualitative and occurs on a non-dichotomous continuum; this fact modifies the concept of healing and treatment at the general medicine level. This article, which is a personal view, aims to delve beyond the usual superficial concepts, to get to summarize and conceptualize some of basic elements of the different ways of understanding the healing/curing process in general medicine. Cure refers to successful treatment; the cure is a process external to the patient that the doctor performs. Healing, in contrast, is an internal process through which the person becomes whole. Although curing and healing are different, healing is contained in care like a Russian doll. Healing is a necessary part of cure; it is actually its deep heart. The three most important concepts to understand the healing process are: 1) The human body; 2) The doctor-patient relationship; and 3) Empathy and self-empathy. These concepts allow us to build different ways of understanding “healing”: A) Cure is transforming emotions; B) Cure is to achieve interconnection; C) Cure is unlocking situations; D) Cure to fully understand the person; E) Cure is modify the patient’s relationship matrix; F) Cure is favouring the patient’s self-healing abilities. Epidemiology and public health tend to focus exclusively on the cure process and quantitative data. But these data is mediated and depends, especially at the level of general medicine, on “caring.” Thus, their interventions at the level of primary health care are erratic and ineffective. The integration of care (personal experience of the disease) and cure (objective physical manifestations) processes in public health and epidemiology would make it possible to develop and innovate practices and organizational models that can improve care processes.
Key Words: General Practice; Framework: Health; Cure; Patient-Centered Care; Physician-Patient Relations
The words "care and cure" or "medical care and cure" indicates the clinical work function of the physician, and also expresses an employment context of the professional role. Technological progress and the fragmentation of treatment lead to a conception of assistance limited to organic factors at the expense of forgetting psychosocial factors. The hierarchical pyramidal structure of the health organization helps to consolidate the impersonal character of the care and cure process, giving more importance to the mysticism of care based uncritically on the organic predominance with respect to the psychic. The conception of the person as a global entity and the consideration of the individual as a being endowed with emotions do not fit in this healthcare model (1).
The usual biomedical approach to "cure" is to consider that the general practitioner (GP) does this through medication; this approach is generally is defined in quantitative terms (e.g., "90% of cases are said to resolve at the GP level"), and is considered dichotomous (cure: yes / no). However, one can think differently, so that the sense of healing / resolution is qualitative and occurs on a non-dichotomous continuum. Many diseases in general medicine are self-limiting and "cure" on their own, or are chronic and have no "cure"; This fact modifies the concept of healing and treatment at the general medicine level; Thus, among other things, this concept may suppose that many of the medical pharmacological treatments are useless (2).
Thus, in a context of biological assistance, the disease tends to be considered an organic event isolated from the total context. But, at the other extreme is the danger of "psychologization" that also brings about the consequent deformation of the professional relationship: in this approach the disease is seen only in terms of psychological conflicts. In this way, the form is changed, but the substance of the doctor-patient care relationship remains deformed and essentially unchanged (1).
"Cure" or "treating" without "scientific" evidence can be a loving or well-intentioned action, but not medicine, and it can be dangerous. But science without caring for the patient empties medicine of its content and opposes its potential to help the sick. Thus, the two components are essential to the "art of making medicine." It can probably be said that medicine is a discipline based on humanism. Compassion is an essential component of high-quality healthcare in today's technological world of medicine. Probably true is the aphorism that more errors have been made in medicine by those who "don't care" for patients than those who "don't know medicine" (3).
Although there are schemes of how to apply a biopsychosocial vision of the care and healing process in practice (4), such descriptions seem to be somewhat superficial, and there is a lack of reflections that deepen, bring to light and clarify basic concepts. In this scenario, this article, which is a personal view, that it is based on an unsystematic or opportunistic search for information and in author's experience, aims to delve beyond the usual superficial concepts, to get to summarize and conceptualize some of basic elements of the different ways of understanding the cure/care process in general medicine.
The comments in this article should be considered as a personal point of view, based on the author's experience during more than 30 years of work in general medicine, plus an unsystematic or opportunistic search for information considering the bibliographic references of selected articles, reviews of books related to the topic, and opportunistic searches on the Internet.
Curing and healing
There is a fundamental distinction between healing and curing that is based on the true patient-centered consultation. Although this difference is at the center of the biopsychosocial paradigm, it is not fully recognized in current medicine. Cure refers to successful treatment; the cure is a process external to the patient that the doctor performs. Healing, in contrast, is an internal process through which the person becomes whole. Healing can occur on the biological / physical level (for example, when a fracture heals), and on the emotional level (for example, when there is a recovery from childhood trauma). Although curing and healing are different, healing is contained in curing like a Russian doll. Healing is a necessary part of curing -it is actually its deep heart (5) (FIGURE 1).
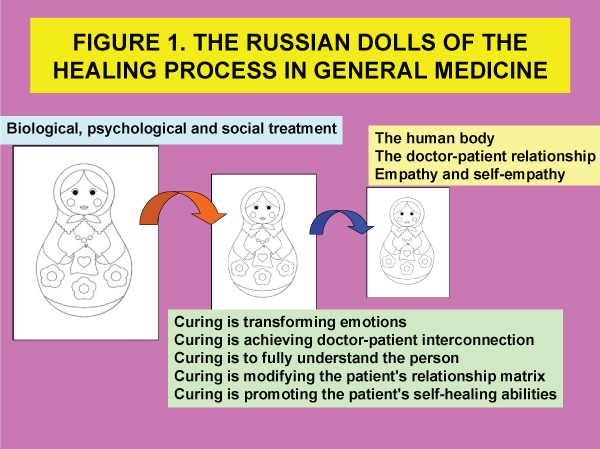
Figure 1: The Russian Dolls of the Healing Process in General Medicine
Starting from the classic concept of the biopsychosocial, medical intervention or treatment can be classified as treatment in the biological dimension, treatment in the psychological dimension, and social treatment (TABLE 1) (4). However, it is convenient to go a little deeper to try to identify the basic elements that give rise to the different ways of understanding the healing process in general medicine. The three most important concepts to understand the healing process are: 1) The human body; 2) The doctor-patient relationship; and 3) Empathy and self-empathy.
Table 1: Classical Dimensions of Medical Treatment.
DIMENSIONS OF MEDICAL TREATMENT |
CONCEPT AND EXAMPLES |
Treatment in the biological dimension |
It refers to the biomedical treatment of the disease, such as the etiological treatment of the cause (for example, antibiotics, or surgery). Medications are used with the expectation that they will achieve a cure, an improvement of the disease process. But, despite these expectations of biological efficacy, it must be taken into account that many drugs also act through the psychological dimension (placebo effect). In addition, medications with proven biological effects may also have adverse effects in the psychological dimension, mediated through the central nervous system or due to their symbolic meaning; thus they can counter-act on the patient (for example, tranquilizers prevent clarity for decision-making or for understanding a situation; Although morphine relieves pain, some patients who fear being addicted, achieve little relief efficacy). Surgery can also have a placebo effect: for many years, in the past, the internal thoracic artery was ligated to treat angina, and it was considered effective, and in fact, many patients reported improvement with it; it was a placebo effect. Some medications and surgical interventions have important interpersonal effects (adverse effects in the psychological dimension), for example hysterectomy favours the idea of sexual impotence in women, etc. |
Treatment in the psychological dimension |
It is mainly aimed at modifying feelings-emotions, functional capacities, and the well-being of the patient. It is especially based on the doctor-patient relationship and its placebo effect. The psychological aspects of taking the clinical history, the physical examination, the request for complementary tests, the prescription of drugs, the successive appointments, etc., and their possible psychological implications must be considered, in order to use them judiciously and deliberately and maximize their benefits beneficial effects. Hospitalization can cause anxiety (loss of control and intimacy...) or be beneficial psychotherapeutically (safe place). Physician reassurance, consisting of a generally optimistic attitude and specific statements based on data or experience, can be helpful if the sources of the patient's fears are known. The simple act of verbalizing emotions can improve chronic anxiety; after such verbalizations, the patient can achieve a new or fresh vision that allows him to face the situation. Judicious advice is another form of psychological intervention. Health education is yet another form of psychological treatment |
Treatment in the social dimension |
Any intervention that involves some environmental change, including changes in contact with the health system (such as hospitalization...), sick leave, the prescription of rest, environmental changes, interpersonal changes in family, school, and work relationships |
The human body / human feelings
The word "body" means what is perceptible with touch and sight. But the human body also includes actions and feelings. The fact of confronting the body with the surrounding reality can lead to ecological pathology, such as anorexia and bulimia as eating disorders; here external world talks to the body. In the work of healing, the professional meets the human body on a daily basis: the body of man and woman, of the child and of the elderly, with differences for social, cultural, genre and ethnic reasons, but with a common element: their fragility in the sense of having a limit associated with their human condition. The sick human body requests care and cure.
The body, especially the suffering body, constitutes significant language. For Freud in the human being the psychic structure has an influence on the organism and this results in the body. The psychoanalytic experience forces us to consider the body not as something given biologically, but as the effect of language on the living; A body that speaks (6). The disease causes a condition of dependency, a feeling of shame, discomfort, and ridicule of the body itself; a feeling of non-self-sufficiency. The patient has to entrust himself to the other, relate to the other for healing (7).
Doctor-patient relationship and care/cure process
Healing is the task of nurturing the other. In the process of care and cure, the relationship with the person assisted is important. The doctor's relationship with the patient is the true core of clinical praxis. This relationship represents the center of the healing profession, but it is not an innate ability, nor is it easy to acquire. The relationship with the other to be cured necessarily involves paying attention to communication and dialogue with the other (7). The GPs se interesan por sus pacientes y sus familias; es la calidad de estas relaciones, junto con la confianza que se construye a lo largo del tiempo con los pacientes, lo que hace que los GPs sean únicos e insustituibles, dando validez a su consejo (8).
The process of cure and care means establishing a device of reception, listening, of silence, of recognition of the other, and establishing a short and long-term bond with the other. The act of healing is full of tenderness and compassion (3) and hope; Hope is truly therapeutic. There is always something worth hoping for in the face of a difficult illness (5).
The doctor-patient relationship model is an element of "curing context creation". There are some nonspecific effects of the doctor-patient relationship on medical intervention: physicians who adopt a warm and patient-friendly consultation are more effective in their interactions with patients than those who adopt a formal style and do not offer friendly security. During the consultation, these more effective physicians take into account the patient's health beliefs, their general opinions on medicine and specifically on the intervention at that time, as well as the complexity of the socio-cultural effects (2, 9). It should be borne in mind that the doctor-patient care relationship is a technical instrument at the service of patient treatment and cure (10-12).
Empathy and self-empathy
Empathy is the distance and proximity to the body that is healing. Empathy in a philosophical and psychological sense can generally be identified with the immediate intuition and emotional involvement of the other's affective state. The sick person has to trust the other. But, there is also a moment in which the encounter with the other corrects and re-defines the professional's own way of life (13). Good communication, free communication between people, is always therapeutic. True communication occurs when the evaluative tendency is avoided, when we listen with understanding. What does this mean? It means that we see what is expressed and the other person's ideas from their point of view. If it is understand the other person in this way, the GP can enter a private world. In this situation the patient can change, and the GP also can change (3). To the extent that we respond emotionally to someone, we respond physiologically to that person. People in an empathic relationship exhibit a correlation with indicators of autonomic activity. The experience of feel cared in a relationship reduces the secretion of stress hormones and shifts the neuroendocrine system toward homeostasis (14).
To improve clinical work in general medicine, a previous and crucial element is necessary “understanding” the patients and ourselves in the respective contexts (13,15). Knowledge and understanding of the symptom -its diagnosis- depends on the doctor-patient relationship. Diagnosis ("evaluation") means discovering what the patient brings and how he sees the problem. The patient also makes a diagnosis (evaluation) of the therapist and her ability to understand and treat her problem. The filter that the GP has in her office changes the way of diagnosis and understanding of the symptom (13). So, these 3 basic elements of: the human body, the doctor-patient relationship, and empathy and self-empathy give rise to various approaches to "healing" in general medicine: A) Curing is transforming emotions; B) Curing is achieving doctor-patient interconnection; C) Curing is unlocking situations; D) Curing is to fully understand the person; E) Curing is modifying the patient's relationship matrix; and F) Curing is promoting the patient's self-healing abilities (TABLE 2).
Table 2: The Basic Elements of The Different Ways of Understanding the Healing Process in General Medicine.
|
BASIC CONCEPTS |
||
Human body |
Doctor-patient relationship |
Empathy and self-empathy |
|
WAYS TO UNDERSTAND THE “HEALING” PROCESS |
Curing is transforming emotions |
||
Curing is achieving doctor-patient interconnection |
|||
Curing is unblocking situations |
|||
Curing is to fully understand the person |
|||
Curing is to modify the matrix of relationships of the patient |
|||
Curing is favoring self-healing abilities of the patient |
|||
Curing is transforming emotions
The task of treatment or "healing" carried out by the GP includes two jobs: a manual-intellectual job, and another emotional job. This emotional work must deal with the person's feelings (7). If the doctor understands that she is helping the patient to “dialyze” her or his anguish, she or he will bear better patient's listening or the fact of not being able to cure the disease. “Curing” can be understood in analogy to dialysis, in which the patient's experience of illness passes through the clinician's compassionate equanimity for affective detoxification and cognitive clarification (14).
Curing is achieving interconnection with the patient
GP to curing have to understand that is involved in helping the other as a person, rather than as a scientist; "Cure" is to achieve a situation of interconnection. Perhaps together, the patient and the doctor can understand the problem. The only way to overcome suffering and turn it into joy is to find its meaning. The suffering patient should, with the help of her/his inner wealth and that of the doctor, be able to turn her pain sensation into an ally (16). The tool / technology of family doctors are the doctor himself. For patients to get better, the most important thing is that they like the doctor. If trust does not become an important part of this relationship, "healing" is unlikely to occur (2). However, trust connection is difficult to achieve, and thus discrepancies about expectations and results of interventions between doctors and patients are constant (17-19). /p>
Curing is unblocking situations
The concept of cure or health problem resolution should be seen in general medicine as a factor that facilitates the unblocking of a situation; change from one environment to another. It is the result of the action that gives rise to a new scenario. Healing takes place through a person's encounter with other people (healing is a "relational" concept, of adjustment or change in the matrix of relationships or connections), rather than through interventions in the body or mind of the isolated individual. Healing implies in one way or another return of the part to the whole (2). The blocking of situations, scenarios or contexts means a danger for the patient. The disease supposes for the patient a deficit, an empty hole, a dead end. These blockages are the ones that must be solved in defence of health. Healing is achieved when the patient can perceive that the situation is different from how he initially perceived it. By becoming aware of the problem globally, treatment can emerge. A healthy person is not one who is free from problems but one who is able to face them (17, 20-22).
Curing is to consider the body in its biopsychosocial totality
Curing is to consider the body as the physical, psychic and spiritual spokesperson for health problems (7). On the contrary, cure in the dominant biologist care model is to cure the somatic symptoms without taking into account the comprehensive evaluation; it is based on the concept of symptom as an isolated entity and not as part of a totality, and of the objective consideration of the disease, but not of the patient. The patient's personal problems are prohibited in the patient's language. Thus, in order not to make “mistakes” in this relationship with the doctor, the patient expresses the psychosomatic as organic symptoms (1). In general medicine, the challenge is to give up the idea of the usual "cure", modifying this concept and its criteria, so that it should focus mainly on relieving, at least in part, some of the many patients’ psychosocial problems (23-25).
Curing is to modify the patient's relationship matrix: connect/disconnect
The disease can threaten, distort or break the patient's sense of connection with others or with the world. It can interfere with her safety; challenge sense of control over her/his destiny. Pain, loss of function and other types of problems decrease the possibilities of contact, increasing the feeling of isolation in daily life (9, 12, 26). The evolution of the disease (change, learning, healing, adaptation, etc.) in a living organism (a person, a patient) always concerns the individual plus its relational matrix. "To be" means to be related, and it means to build or modify those relationships.
When we believe that we intervene in isolated individuals, such as when we treat an organic disease in an individual (pain, alcoholism, obesity, etc.) or treat a mental disorder (which we define as an alteration of brain neurotransmitters) with drugs, we never treat alone to an individual, but changes in that person (relief of pain, improvement of depression, giving up alcohol or smoking, or changes in diet, learning disabilities, etc.) have repercussions on relationships with other individuals and these changes back on the patient, etc. Healing (treatment, GP intervention) is made possible through the therapist's involvement in the matrix of communications and relationships with other people (27, 28).
The concept of healing illness or trauma has to do with avoiding feeling overwhelmed and broken connections. Healing is restoring broken connections. Although the stressful environment of the patient could not be modified (because it is not always possible), the world that surrounds each one (the context of each one), is largely created by oneself, because we are interpreting what surrounds us. Therefore, if we vary the interpretation of what surrounds us, in a certain way, it is as if we varied our environment. Curing (treatment, professional intervention) becomes possible through the therapist's participation in the matrix of communications with other people (17, 21, 22, 29, 30).
Curing is favouring self-healing abilities of patient
Cure is due largely to certain factors of the patient (desire to live, beneficial role of positive emotions, trust in the doctor and cooperative doctor-patient work). The basic goals in this field is to learn enough to be able to create a "healing climate" in which the person's self-healing and self-repairing abilities can be achieved as an aid into medical protocol (31).
Implications of the cure and care process on public health and epidemiology
Public health and epidemiology tend to focus exclusively on the cure process. In the mid-1980s, five major tasks of epidemiology in public health practice were identified: public health surveillance, field investigation, analytic studies, evaluation, linkages, and. policy development (32, 33). It is about identifying the continuous patterns of disease occurrence and risk so that investigation, control and prevention measures can be applied efficiently and effectively. Reports of morbidity, natural history, clinical spectrum, descriptive epidemiology, and disease risk factors are common sources of surveillance data before determining which disease intervention methods might be appropriate; Epidemiologists are used to using quantitative approaches (34), including evaluation of efficacy, effectiveness, and efficiency (35).
However, it is often not realized that what appears to be a systematic approach is biased; the data of "curing" are mediated and depend, especially at the level of general medicine, on "caring." Public health and traditional epidemiology do not usually understand the difference between curing and healing: healing refers to the personal experience of the disease, unlike cure which refers to its objective physical manifestations (36). To promote and generate comprehensive epidemiological information that can truly improve the health of the community, both the classic quantitative epidemiological approach on “curing” and the qualitative one on “caring” are necessary. The integration of care and cure processes in public health and epidemiology would make it possible to develop and innovate practices and organizational models that can improve care processes. All this in order to be able to respond to the reference population with quality health and social care. TABLE 3 shows an approach to this concept from general medicine (37).
Table 3: Implications of the Concepts of Care and Cure in Epidemiology at the Level of General Medicine.
DIMENSIONS |
RESEARCH METHOD |
LEVEL OF GENERAL MEDICINE |
||
Current context of the person |
Recent context of the person |
Background of the person |
||
CARE |
PREDOMINANTLY QUANTITATIVE |
-Symptoms and physical signs |
-Onset and change of symptoms and signs |
-History of disease |
CARE |
PREDOMINANTLY QUALITATIVE |
-Reason for consultation |
-Changes in the mental situation and in behavior and habits |
-Personality traits |
Sense of curing/health problem resolution is qualitative and occurs on a non-dichotomous continuum; this fact modifies the concept of healing and treatment at the general medicine level. Cure refers to successful treatment; the cure is a process external to the patient that the doctor performs. Healing, in contrast, is an internal process through which the person becomes whole. Although curing and healing are different, healing is contained in curing like a Russian doll. Healing is a necessary part of curing. The three most important concepts to understand the healing process are: 1) The human body; 2) The doctor-patient relationship; and 3) Empathy and self-empathy. These concepts allow us to build different ways of understanding "healing." Epidemiology and public health tend to focus exclusively on the cure process and quantitative data. The epidemiologist as a scientist seeks the "end" of things; the GP, for its part, wants to establish the “principle”. The integration of care (personal experience of the disease) and cure (objective physical manifestations) processes in public health and epidemiology would make it possible to develop and innovate practices and organizational models that can improve care processes.